 |
|
|
|
Surgical Treatment of Gastric Dilatation-Volvulus (GDV)
Howard B. Seim III, DVM, Dipl. ACVS
Fort Collins, CO
Key Points
• GDV patients are saved in the presurgical management
• Patients referred for surgery should be decompressed prior to referral and during transport
• Gastropexy techniques result in permanent pexy
• Ventricular tachycardia is common postoperatively
• Gastric necrosis signals a grave prognosis
Presurgical Treatment
Introduction
Patients with GDV are considered critical cases; every minute of presurgical treatment is vital to a successful outcome. Survival is generally determined by early and appropriate presurgical management; not surgery. Efficient presurgical treatment usually involves a minimum of two people. Both gastric decompression and shock therapy should be done simultaneously. If this is not possible; decompression should be performed first. It is stated that gastric decompression is the single most important factor in reversing cardiovascular deficits in patients with GDV.
Decompression
Generally, orogastric intubation can successfully be performed 80 - 90% of GDV patients. Decompression vial orogastric intubation should be attempted in all cases.
Technique
The stomach tube is measured to the last rib and marked with a piece of tape. A stiff foal or mare stomach tube with a smooth tip works best (having several diameter and stiffness tubes is ideal). Apply adequate lubrication to the tube. Place a functional mouth speculum; generally a roll of 2" tape secured in the mouth with tape encircling the muzzle. As the stomach tube is passed, you will generally meet resistance at the esophageal-stomach junction. Pass the tube firmly in a twisting manner to pass the lower esophageal sphincter.
If you are unsuccessful, place the patient in various positions and attempt to pass the tube (i.e., elevate animal at 45 degree angle with rear feet on floor and forefeet on table, right lateral recumbancy, and left lateral recumbancy). This movement may encourage the stomach to rotate enough to allow tube passage. Be careful not to position the patient in dorsal recumbancy as this will increase abdominal visceral pressure on the caudal vena cava.
If still unsuccessful, try different diameter tubes; start with a smaller diameter, more flexible tube and proceed as described above.
If still unsuccessful, attempt to remove some of the air in the stomach by placing a l6 or l8 gauge needle at the point of distention in the right flank region. Ping the area to make sure the spleen is not under the proposed trocarization site. After trocar decompression, attempt to pass the stomach tube as described above.
If still unsuccessful, sedate the dog with a narcotic (Oxymorphone .11 to .22 mg/kg IV) and try to pass the tube again. Mild sedation is recommended if the patient strongly resists physical restraint.
Success in passing a stomach tube depends on the skill of the operator and available assistants.
If you are successful at passing a stomach tube, but plan to refer the patient to a referral surgical center for gastropexy, transport the patient with the tube remaining in the stomach (i.e., taped to the mouth) or bring the tube out through a pharyngostomy as described below.
a. Orally palpate the fossa lateral to the hyoid apparatus until a lateral bulge is seen.
b. Make a small skin incision over the bulge and press a curved forceps (substitute for finger) through the soft tissues and skin incision.
c. Pull the stomach tube through the incision with curved forceps; then pass the tube over the arytenoid cartilages, down the esophagus, and into the stomach (measure to the 13th rib).
Disadvantages include: heavy sedation or general anesthesia is necessary for placement of tube.
If still unsuccessful - a temporary gastrostomy can be performed. The patient is placed in left lateral recumbancy with the right flank area clipped and surgically prepared. Heavy sedation and local infiltration of lidocaine or light general anesthesia is performed. A 4 - 5 cm incision is made in the skin over the point of greatest gastric distention (generally 1 - 2 cm caudal to the 13th rib and 2 - 3 cm distal to the transverse processes of the lumbar vertebrae). A grid technique is used to gain entrance into the peritoneal cavity. Due to severe gastric distention the stomach wall is pressed against the abdominal wall and easily identified through the flank incision. The stomach wall is sutured to the skin using a simple continuous pattern with 3-0 Maxon. This is done prior to incising into the stomach lumen. A #11 BP scalpel blade is used to puncture into the lumen of the stomach. Gas and stomach contents are expelled under pressure so stand back! The gastric mucosa is evaluated for viability.
Disadvantages of gastrostomy include: the stomach is sutured in its rotated position and more time is required when definitive surgical treatment is performed due to the necessity of closing the gastrostomy.
Shock
Once the stomach tube has been passed into the stomach or gastrostomy performed, the stomach is lavaged with warm water. If a stomach tube was successfully passed, the stomach contents should be evaluated for color and presence or absence of necrotic gastric mucosa. This may give an impression of gastric viability.
Fluids
Shock dosage of polyionic isotonic fluid is administered to expand the vascular compartment. For convenience, lactated Ringer's is generally used. One or two indwelling catheters are placed and 90 cc/kg rapidly infused. Clinical signs are monitored and fluids continued appropriately. In most cases that are adequately decompressed, shock will rapidly be reversed.
Hypertonic saline/dextran
Using a GDV model to study the effects of small-volume (5 ml/kg) 7% NaCl in 6% dextran 70 (HS/D70) as an alternative to shock dose of 0.9% saline as a treatment for GDV shock, it was shown that 5 minutes of HS/D70 at 5 ml/kg followed by surgical maintenance of 20 ml/kg/hr was more effective than a 60 ml/kg 0.9% saline over a 60 minute period followed by surgical maintenance of 20 ml/kg/hr. Resuscitation was better sustained with small-volume HS/D70 compared with conventional large volume 0.9% saline.
Corticosteroids
Corticosteriods have been shown to be useful in hypovolemic shock by stabilizing lysosomal membranes, increasing cardiac output, and helping to maintain integrity of the circulatory system. For endotoxic shock, steroids reduce serum levels of endotoxin, promote clearance by the reticuloendothelial system, and interfere with induced immune reactions by decreasing complement fixation. Dexamethasone at 4 mg/kg is a widely accepted regime.
Flunixin meglumine
Endotoxemia plays a critical role in the pathologic alterations associated with GDV however, administration of flunixin megulmine after onset of gastric dilatation-volvulus may be too late to block the rise in plasma prostacylin concentration, but will prevent additional rise and, therefore, attenuate the effects of endotoxemia. Flunixin meglumine should never be given with steroids or for more than 2 days.
Deferoxamine
Reperfusion injury occurs when transiently ischemic tissue is reperfused with normally oxygenated blood, thereby generating free radicals from xanthine oxidase-dependent pathways. Molecular oxygen introduced during tissue reperfusion combines with xanthene oxidase and results in production of superoxide radicals. Normal cellular defense mechanisms are quickly overwhelmed. Cellular injury occurs from lipid peroxidation of cell membranes, destruction of enzymes, and cleavage of DNA; all resulting in cellular death. Therapy for reperfusion injury is directed at inhibiting xanthine oxidase, destroying superoxide, free radical scavengers, and iron chelators that prevent chemical reactions producing hydroxyl radicals (the most damaging of the free radicals). Various substances have been studied but either are not effective or have not yet been released for clinical use: allopurinol, superoxide dismutase, iron chelators (deferoxamine), free radical scavengers (catalase, DMSO, mannitol). Prospective randomized clinical trials are needed to determine the effectiveness of reperfusion injury prevention on the mortality and morbidity associated with GDV.
Antibiotics
Bacteriocidal antibiotics have been advocated in the treatment of hypovolemic shock patients. They help reduce bacterial numbers and thus endotoxin elaboration, and aid in prevention and treatment of peritonitis caused by possible gastric ischemia and necrosis.
The surgeon should be aware that appropriate presurgical medical management is critical to patient recovery (i.e. treatment of shock and subsequent stabilization).
Surgical Treatment
Surgical procedures utilized in the treatment of gastric dilatation-volvulus can be divided into two categories; 1) immediate decompression and 2) therapeutic (or prophylactic) gastropexy. Immediate decompression is performed with a successfully passed stomach tube secured to the patient or temporary gastrostomy as described above. Therapeutic or prophylactic gastropexy techniques are described below.
Gastric repositioning:
Anatomic repositioning of the stomach is necessary to prevent recurrence of GDV. Repositioning will sometimes occur spontaneously at the time of decompression. Knowledge of normal anatomy is necessary to understand how repositioning is performed. In each case the same maneuver is performed to derotate the stomach. The pylorus, located near the cardia of the stomach, is grasped with the right hand and elevated as the left hand presses down on the fundus of the stomach. Reduction is easily performed if the stomach has been decompressed. The spleen usually will be carried back to its normal location when the stomach is derotated. Exteriorizing the spleen may facilitate derotation of the stomach. Spleenectomy is rarely performed, but may be necessary if spleenic vessels are infarcted. The greater curvature of the stomach is examined for areas of necrosis. If necrosis is present, the prognosis is unfavorable to grave.
Gastropexy Techniques
Belt Loop Gastropexy
This technique is based on the construction of a sero-muscular antral flap attached around a segment of transversus abdominus muscle. A horseshoe shaped incision is made in the serosal layer of the antral portion of the stomach with its base at the greater curvature. The sero-muscular portion of the stomach is identified by grasping the full thickness of the antral wall between the thumb and index finger and "slipping" the mucosal layer away so only the sero-muscular portion of the wall remains between thumb and finger. The sero-muscular layer is incised with scissors and the horseshoe shaped sero-muscular antral flap is dissected and elevated of the submucosal layer. The stomach is replaced in the abdominal cavity in normal position and the sero-muscular flap lined up with the transversus abdominus muscle. Once this optimal location is discovered, two longitudinal incisions (along the fibers of the transversus m.) are made in the transversus abdominus m. The segment of muscle between the incisions is undermined. The sero-muscular flap from the stomach (i.e., belt) is passed through the transversus abdominus m. (i.e., loop) and sutured to itself to complete the "Belt-Loop" gastropexy. 2-0 monofilament absorbable synthetic suture in a simple interrupted pattern is used to secure the flap in place. Advantages of belt loop gastropexy include: it is relatively easy to perform alone and in the middle of the night, it can be performed quickly, and it is an effective means of permanent gastropexy.
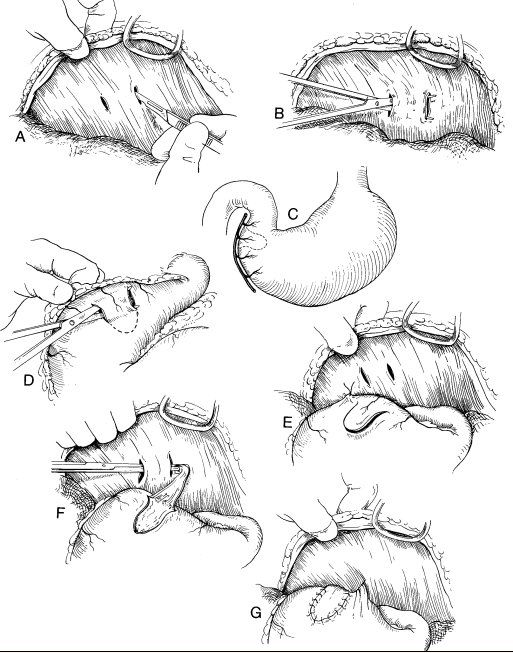
Circumcostal gastropexy
Stay sutures are placed approximately 4 cm apart on the ventral pyloric antrum.
An "I" shaped incision (approximately 2/3 the length of the antrum) is made in the sero-muscular layers with the long axis of the "I" parallel with the long axis of the antrum. Two sero-muscular flaps are elevated; note that the submucosa and mucosa are not penetrated. The flaps are approximately 3 cm long and 1-1.5 cm wide. One of the last 4 costal arches on the right is exposed by sharply incising and reflecting the musculature for approximately 5 cm at the costochondral junction. NOTE the diaphragm attaches very close to this point and caution must be taken to avoid creating a pneumothorax.
Stay sutures are placed in the sero-muscular flap, the flap is carried around the exposed costal arch, and sutured to each other using simple interrupted 2-0 synthetic absorbable suture. Advantages of circumcostal gastropexy include: the lumen of the stomach is never entered and the gastropexy is permanent.
Postoperative management;
Usually 3-4 days of intensive monitoring and treatment is necessary for the successful treatment of GDV.
a. Shock is a postoperative possibility and the patient should be monitored and treated accordingly.
b. The patient should be held off food and water for 24 hours following surgery. During this time maintenance fluids should be supplied by 66 cc/kg/day of a polyionic isotonic crystalloid fluid. Vomiting may occur following surgery; the NPO period should be extended accordingly. Gastritis and gastric motility disorder are common sequelae to GDV.
c. After 24 hours of no vomiting, oral alimentation should begin gradually with a sequence of ice cubes, water, baby food and finally canned dog food. This should occur over a 2-3 day period.
d. Antibiotics should be continued for at 7 - 10 days.
e. Routine surgical complications such as infection, dehiscence, seroma, etc. should be watched for and treated accordingly.
f. EKG monitoring: the most common severe postoperative complication is cardiac arrhythmia's. Approximately 75% of GDV's will developed severe arrhythmia's in the postoperative period. Arrhythmia's can be present at the initial time of presentation but most often occur within 24 hours of surgery. Ventricular premature contractions, progressing to ventricular tachycardia is most common. Etiology is unknown but shock, hypoxia, acid base alterations, endotoxins, MDF, reperfusion injury, release of free radicals, and hypokalemia have been associated. A total body potassium deficit has been recently proposed. Etiology includes anorexia, vomiting, tremendous outpouring of potassium rich fluids into a dilated stomach, and use of potassium poor fluids in the treatment of shock. For this reason, adding 20-30 mEq of potassium chloride per liter of maintenance fluids during and after surgery are recommended.
|
|
|


Copyright ACVC