MVZ Esp. MCP y G . Javier Del Angel Caraza
Hospital Veterinario para Pequeñas Especies, Facultad de Medicina Veterinaria y Zootecnia, Universidad Autónoma del Estado de México
Introduction
The micturition can be defined as the mechanism that regulates the exit of urine from the bladder across the urethra in specific periods, event that implies the alternation of the storage phase (or continence) and the emission phase (or emptiness), by means of the activity of the smooth musculature governed by the autonomous nervous system. Nevertheless it is a conscious act that is subject to a high degree of voluntary control.
That is why any problem in these phases generates alterations in the micturition; alterations in the storage phase generates urinary incontinence and any alteration in the emission phase could generate urinary retention. The urinary retention can be defined simply as the lack of emptiness or the incomplete emptiness of the urinary bladder. The residual volume post micturition is from 0.2 to 0.4 ml/kg in healthy dogs (usually <10 ml total in a dog of 15 kg). The majority of the affected patients possesses a residual raised post micturition urinary volume and presents to the palpation a plethora bladder.
The neurological alterations that generate urinary retention rarely concern only the urinary tract, since in the majority of the cases it is secondary to injuries of the High Motor Neuron (cranial injuries to the 4th Lumbar in dogs) commonly with clinical evident signs as the paraplegia or tetraplegia with increase or normality of the reflexes of the members. Nevertheless occasionally patients appear with a plethora bladder difficulty to empty, without evident signs of neurological injury or obstruction, situation beyond the common called idiopathic detrusor urethral dyssynergia. Other common reasons of the urinary retention are the urethral obstruction for diverse reasons as uroliths, matrix stoppers, tumors or urethral stenosis.
Micturition Control
The micturition happens as a simple reflex in newborn animals; nevertheless the reflex is modified by the maturity of the individual until having a voluntary action. To understand the normal neurophysiology of the micturition is necessary the evaluation of the patient and a design for a therapeutic plan adapted to the disorders of the micturition. The micturition is controlled by a number of complex and countless neurophysiologic centers, routes of neurons and neurotransmissions that control both functional units of the micturition: the bladder like unit of storage on having relaxed and on having contracted to increase the intravesical pressure to initiate a process of emptiness and on the other side the urethra that on having contracted supports the continence and on having relaxed serves as a route of conduction for the urine emptiness. The coordination of these structures is possible thanks to the intervention of diverse factors as the central, sympathetic controls and parasympathetic autonomous system and somatic nervous system necessary for the complete voluntary and coordinated emptiness. So the neurological control of the micturition is capable to suffer injuries to different levels.
During the phase of storage or continence the urinary bladder remains relaxed and slowly adapts to the filling due to the activation of the β-adrenergic receptors generated by autonomous sympathetic route by the hypogastric nerve towards the β-activated receptors in the bladder and simultaneously generating the excitation of the β-adrenergic receptors in the smooth muscle of the urethra. Additionally the resistance of the exit of the flow can be owed by a rapid contraction of the striated musculature of the urethral sphincter. As the volume and the vesical pressure increase, the expansion receptors are activated and recounted sensors as information towards the efferent nerves via pelvic nerve towards the brain. The additional nervous completions in the bladder submucous that project the sensation via hypogastric nerve and sympathetic tracts. The resistance of the exit of a normal animal is mediated for the α-adrenergic receptors.
In short, the importance of the components of the phase of emptiness or elimination include (1) the sensation of filling is perceived to central level, (2) the voluntary central initiation of the micturition and the initial relaxation of the urethral sphincters, (3) the stimulation of the pelvic nerve fibers of the pacemaker stimulated across the muscle detrusor, (4) the rapid transmission of the neuromuscular impulses across the bladder creating a coordinated contraction of the bladder and (5) the inhibition happens at local and spinal level by the smooth and striated muscle of the extern and intern urethral sphincters to facilitate the complete emptiness.
When it happens an alteration in any of these steps, it generates an incomplete emptiness and urinary retention.
Physiopathology
From the clinical point of view, the alterations of the micturition (AM) divide in alterations in the emptiness phase that as a rule are demonstrated with urinary retention (RU) whereas those of the storage phase are in the habit of being characterized by the urinary incontinence. The patients with disorders in the phase of emptiness can present RU or paradoxical incontinence.
Diagnostic plan
It is necessary to have a good clinical history doing emphasis in some traumatic incident, description is necessary for micturition pattern. In the young patients it could be owed to congenital pathologies, whereas the adults can be for acquired processes. The males have a very major trend than the females to experiencing mechanical obstructions. It is necessary to do a physical general examination in order to detect alterations in the size, shape, consistency, tour, contour, nodules, uroliths, thickness of the wall and any another alteration. During the physical examination also it is necessary to look for indications of the bladder and the urethra functional condition, with the simple observation of the patient during the micturition or attempts for urinating and the determination of the residual volume of urine after the evacuation. In addition, the urodynamic variables can be estimated determining the relations of pressure and volume that appear during the palpation and manual compression of the bladder.
A neurological complete examination is a special attention in injuries of NMA and NMB: A full bladder, difficulty to empty with the manual compression, partial emptying and a great residual volume, and a spastic urethral sphincter suggests an alteration in the NMA, for cranial injuries to S1 (from brain to lumbar 4).
Alterations in the NMB originate injuries that neurologically interrupt the local sacral arch reflex. Originating an atonic bladder with incomplete spontaneous emptying and easy total voidance with manual compression. The anatomical possibly implied site is the sacral marrow, cauda equine, or bilateral injury of the pelvic nerve.
The patients with detrusor areflexia of neurological origin must be classified as normal, increased or diminished urethral sphincter tone, being based on the facility to empty the bladder manually; as well as the myogenic areflexia for history or presence of urinary obstruction and idiopathic detrusor urethral dyssynergia with the utilization of urodynamics studies and response to the treatment.
The evaluation of results of laboratory tests, as CBC, general examination of urine and biochemical serum profile (that in the opinion of the doctor is necessary), they are in the useful in the diagnostic investigation of all the patients who present a disease of unknown reason. Nevertheless, the metabolic abnormalities that can arise in the patients with urinary retention are important and sometimes risky problems for their life.
The imaging studies are indicated for AM's identification, especially when the problem is given by an exaggerated resistance to the flow of urine evaluating the size, the shape and position of the bladder, the urethra and prostate. The simple studies can demonstrate radiodensity calculus and prostatomegaly. Nevertheless, the studies with contrast mediums are necessary with some frequency, to confirm the injuries in the vesical wall, urethra and some intramural abnormalities. The evaluation of the lumbosacral and sacral coccygeal regions is also important to determine some injury that affect the vertebral column.
The invasive technologies like the cystoscopy in occasions are necessary for the definitive diagnosis of the pathologies promoting the AM. The cystoscopy examination can be realized in some dogs and it contributes a method for the inspection of the bladder, the urethra for abnormal contents and the intramural injuries. During these procedures, samples can be obtained for biopsy. The exploratory celiotomy is indicated for the examination, the capture of samples or the correction of the problem of the urinary tract. The exploratory laminectomy with biopsy or removal of masses, is necessary for the diagnosis, treatment of masses and injuries of the nervous roots.
The cystometrography, manometer urethral profile and electrophysiological studies of the urethra: are urodynamic tests that measure up relations of pressure, volume, flow of the bladder and the urethra during the different phases of the micturition, contributing objectively with information to describe the vesical or urethral dysfunction quantitatively, but it is difficult that an etiologic diagnosis is established definitively. These need special devices and skills, being not very accessible.
Urinary retention
The reasons of urinary retention can qualify in two categories: Neurogenic (detrusor areflexia and detrusor urethral dyssynergia) and not neurogenic (excessive resistance to the exit for uroliths, matrix stoppers, stenosis, tumors, etc.).
The detrusor neurogenic areflexia disorders or idiopathic detrusor urethral dyssynergia, are caused by injuries that affect the arch reflex of the micturition. The injuries of the NMA and NMB can be guilty of an abnormality in this one is the one provoking a RU.
The injuries of the nervous central system, from the cerebellum up to the segments L7 of the spinal cord can produce detrusor areflexia with hyper reflex of the urethral sphincter producing urinary retention; a bladder being observed full, difficulty to empty with manual compression, with perineal normal or hyperactive reflexes.
The injuries of the cerebellum, spinal cord, or traumatism of the pelvic plexus that do not injure the pudendal nerve, can cause detrusor areflexia with a normal tone of the urethral sphincter; observing a disability of micturition, the distended bladder easy to empty with the manual compression and normal perineal reflexes.
In the injuries that affect the marrow segments, or the nervous roots from S1 to S3, pudendal or pelvic nerve; does not exist a micturition or defecation reflex and the urethral sphincter is relaxed, the bladder fills with urine until the intravesical pressure overcomes the resistance and exit generating a paradoxical incontinence, in this moment an hyperflow escapes towards the urethra. The patient does not demonstrate desires to urinate but it leaks, urinates involuntarily or empties his bladder in partial and passive form. It can be emptied easily by manual compression.
The detrusor urethral dyssynergia is defined as the loss of coordination between the contractions of the bladder and the easing of urethral sphincter during the phase of micturition. The etiopathogenesis is not known, but it is believed that it is the result of a partial injury of the cranial NMA to the sacral spinal cord or injury in the urethral or vesical innervations, being able to demonstrate urinary retention, paradoxical incontinence, stranguria and pollakiuria.
The long over distention of the bladder, whose origin can provoke secondary detrusor or myogenic areflexia classified by some authors, provoked by a disruption of the hermetic unions between the fibers of the smooth musculature of the bladder, bothering with the coupling excitation-contraction of the detrusor muscle, giving like result a weak contraction.
Medical managing of the Urinary Retention
For the treatment of the RU there must be established two principles of initial importance:
1. Try to control the abnormalities that imply the risk of the life of the patient, such as: the posrenal azotemia, hyperkalemia and metabolic acidosis. The appropriate therapy of fluids must be initiated for the treatment of the metabolic complications of the RU, as well as the antibiotic therapy and necessary medicines.
2. As soon as possible, it is necessary to do the total emptiness of the bladder. Because the delays can provoke potentially serious complications, as the infection of urinary low tract, metabolic disorders, myogenic detrusor areflexia, hydroureter and hydronephrosis or vesical necrosis principally in cats.
In the treatment of the neurogenic detrusor areflexia, is necessary the medical or surgical treatment adapted for the neurological disease responsible for the RU, the evacuation of the bladder at least three times a day, except when the hypertone of the urethral sphincter prevent the manipulation, the manual compression, is the favorite method.
When hypertone of the urethral sphincter exists, the aggressive manual compression will have to be avoided, due to the fact that it is ineffective and can provoke a traumatism or bladder breaking; in this case it is preferred the intermittent catheterization that is preferable to the permanent one in order to reduce the traumatism of the urethra and the bladder, diminishing the possibility of infection of the low urinary tract.
To produce an easing of the smooth musculature is advisable the antagonist α-adrenergic administration as the Nicergoline (1-5 mg total every 8 hrs PO, in both species) in combination with skeletal muscle relaxes like the Diazepam (dogs 2-10 mg every 8 hrs and cats 2-5 mg every 8 hrs for PO).
When neither the smooth musculature nor the skeletal musculature relaxing is effective, it is advisable the combination of these agents. If reflex of the detrusor exists and but it is insufficient to induce a suitable evacuation, it is possible to stimulate the contraction of the bladder using some Prokinetics as the Cisapride (dogs 0.1-0.5 mg/kg c/8-12 hrs. and cats 2.5-5 mg total c/8-12 hrs for oral route) or Metoclopramide (0.2 to 0.5 mg/kg c/6-8 hrs. both in dogs and cats), which promotes but does not initiates the detrusor reflex. These medicine they must not be in use in presence of urethral hypertone; except in combination with antagonists of α-adrenergics and relaxing of the skeletal muscle (See Figure 1).
In the treatment of the detrusor urethral dyssynergia, it is necessary to try to relax the urethra without disabling the reflex of the detrusor muscle, by means of a treatment to the smooth or skeletal musculature of the urethra and in some cases is necessary the combination of prokinetic and relaxing of smooth and fluted musculature.
In the majority of the patients with normal activity of the detrusor and functional obstruction; after eliminating the mechanical obstruction, the constant myogenic detrusor areflexia being a problem that is controlled by an urethral catheterization during a period that changes from 4 to 14 days, which it can be of great help the medication with cholinergics as the relaxing ones of smooth and fluted musculature.
The not neurogenic RU type will need of the managing of the primary reason and in the majority of the cases it is realized by means of surgical techniques like the cystotomy, uretrotomy, etc.
| Figure 1. Sites of action of the medicaments used in the alterations of neurogenic origin. | 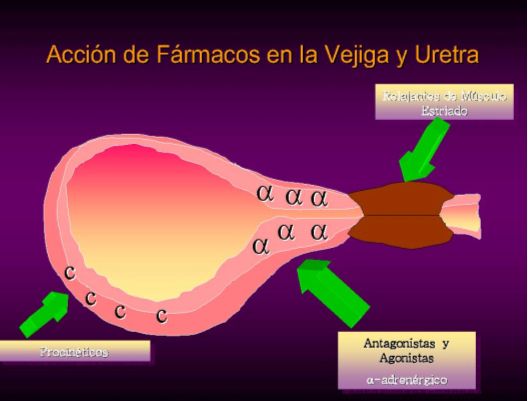
|
|
| |
Complications of the Urinary Retention
Many of the complications of the RU depend on the etiology, speed of the beginning and magnitude of the obstructive pathology. The complete or sudden urinary obstruction generates postrenal azotemia and uremia; a group of metabolic and clinical abnormalities that normally are fatal in 3-5 days if the problem is not corrected. The metabolic complications of the AM are: the azotemia, the electrolyte and acid - base disturbances can turn out to be fatal. The immediate attention of these alterations includes the fluid therapy, to correct the deficiency of the extracellular volume, the hyperkalemia, the acidosis and other metabolic abnormalities.
Unlike the complete obstructions, the partial ones are in the habit of being chronicles. When the partial chronic obstruction induces an exaggerate pressure, the urinary tract can expand progressively up to causing hydroureter and hydronephrosis. The damage of the renal parenchyma can be sufficient to cause renal insufficiency. The RU also increases the predisposition of suffering a low urinary tract infection.
Principally in cats and in some dogs it is possible to present vesical necrosis because of the walls ischemia due to an extreme slimming that does not allow the blood flow to the organ. There is an evident friability of the tissue and very frequently the rupture or urine leak through a small open orifice due to the vesical expansion by urine (See Image 1).
| Image 1. Vesical necrosis in a cat that presented vesical distension by urinary retention due to matrix stoppers. | 
|
|
| |
Control of the micturition alterations complications
The suitable antibiotic therapy must begin when a urinary tract infection is present.
In case of necrotic bladders the signs of uroperitoneum will present principally in patients that even after a cystocentesis handling or perforation by a catheterization with rigid urethral probes and the presence of no controlled urinary retention that generates that the orifice to open by the vesical distension and an escape of urine is generated; it is indispensable to evaluate the integrity of the bladder (for ultrasonography).
Normally the leakage places will be small perforations with a diameter of a 21 hypodermic needle. In the experience of the author it is not advisable to realize a surgical correction since the walls of the bladder are very fragile and in the majority of the cases is impossible to put a stitch since the wall crushes. For what is recommended to drain only the urine of peritoneal cavity (the chemical peritonitis is not so serious as to be handled surgically) having an infectious cystitis the case evaluation and of being necessary realize a surgical wash. And place an urinary soft probe of preference 6 or 8 French calibers (Feeding probe Levin type) with the top up to the vesical trigone only with the purpose of supporting this empty bladder preventing from being distended and hereby having time for a vesical wall regeneration takes place, which will be carried out in a space of 5 to 7 days. In few cases a bladder necrosis exists where tissue feasibility will not exist already and there will not be much to do for the patient. In very serious cases like the one showed in the image 1 maybe is necessary to wrap the bladder with omentum to facilitate the blood flow as last alternative to try to keep the bladder viable; of not being feasible it is possible to resort to rescue surgical skills as it is the derivation of the ureters towards the skin or the colon.