Dominique J. Griffon, DMV, MS, PhD, DACVS, DECVS
Associate Professor, Head, Small Animal Surgery Director, Laboratory for Orthopedic Research on Biomaterials University of Illinois, Small Animal Clinic
Urbana, IL, USA
Disease of the medial coronoid process is a leading cause of osteoarthrosis of the canine elbow. The ideal candidate for surgical treatment of a fragmented coronoid process (FCP) is a dog under 12 months of age with clinical and radiographic signs of FCP. Surgery is also indicated in mature dogs, especially if DJD is absent or minimal. Once severe DJD is present, conservative management may be as beneficial as surgery.
This presentation will focus on current controversies surrounding the treatment of coronoid disease and associated conditions of the elbow. Videos of clinical cases will illustrate the components of arthroscopic management of FCP in dogs.
Is Arthroscopy Superior to Arthrotomy When Managing FCP?
Excision of FCP has traditionally been performed via a medial approach to the elbow. Although several approaches have been described, the intermuscular approach is technically easier and associated with less morbidity. The approach is slightly more complicated that that the caudo-lateral compartment of the elbow, but does not require specialized instruments. Potential complications include inadvertent transection of the medial collateral ligament or median nerve. This approach provides limited exposure to the joint.
Recent advances in arthroscopy have greatly improved our ability to explore and treat elbow disease. In fact, this technique has allowed the identification of variation in appearance of FCP:
 Fragment on the medial margin of the MCP
Fragment on the medial margin of the MCP
Erosion of the lateral rim of the MCP
Incomplete fragmentation (fissure)
Fragment in situ (arrows)
Minimally migrated FCP
Fully migrated FCP (joint mouse)
Chondromalacia--eburnation of the MCP
The disadvantage of this technique consists in the equipment and technical expertise required to perform this treatment. A 2.7mm arthroscope may be used in large breeds, although atraumatic insertion of the scope between the humeral head and the ulna may be difficult, especially in dogs with radio-ulnar incongruity. A 1.9mm 30° fore obliqued scope is therefore preferred. The entire joint is first explored through a medial portal, including the anconeal process, both coronoid processes, the humeral condyle and radial head. The main advantage of arthroscopy is that it provides unparalleled visualization of the joint in a minimally-invasive manner, thereby decreasing post-operative morbidity. One study found no difference in post-operative gait analysis of normal dogs undergoing arthroscopic versus open exploration of the elbow (Bubenik LJ et al, 2002). However, two other studies documented improved function in dogs immediately after and over the 21 months following arthroscopic treatment of FCP, compared to arthrotomy (Schwarz et al. 1993, Meyer-Lindeberg A et al. 2003). Arthroscopic management of FCP therefore appears to minimize post-operative pain compared to open arthrotomy, but further studies are needed to long term benefits on degenerative joint disease.
Arthroscopic Excision of FCP or Arthroscopic Subtotal Coronoidectomy?
| Figure 1. | 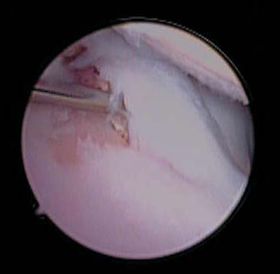
Arthroscopy of the elbow of an 18 month old German Shepherd with elbow dysplasia. Note the eburnation of the medial coronoid process and lesion of the opposing articular surface of the humeral trochlea. This dog was treated via subtotal coronoidectomy and micropicking of the "kissing" lesion of the humerus. |
|
| |
FCP has traditionally been treated by excision of the fragmented portion of the medial coronoid process. This may be achieved arthroscopically, via insertion of a grasping forceps or shaver through a triangulated cranio-medial instrument portal. The sclerotic subchondral bed is subsequently debrided. A subtotal coronoidectomy has recently been proposed for the treatment of dogs with FCP (Fitzpatrick N, 2005). The technique can be performed via a limited medial approach or via craniomedial triangulation of a small osteotome, angled from the caudomedial border of the medial portion of the coronoid process to the craniolateral margin of the radial incisure. Although the author noticed a progression of DJD on radiographs, only 2% of 31 dogs followed for 3 years after surgery had recurrence of lameness. Histopathology of the coronoid processes removed in this study confirmed the presence of subchondral fissures extending beyond the area of visible cartilage damage. While these findings support the concept of a subtotal coronoidectomy, one could argue that these fissures could have healed if the biomechanical loading of the joint had been altered. The effectiveness of the procedure was attributed to the complete removal of diseased cartilage and subchondral fissures, eliminating the need for cartilage healing in a contact environment and unloading the medial aspect of the humeral condyle. If this procedure decreases pressure across the medial compartment of the elbow, it does not fully align the articular surfaces of the ulna and radius in dogs with radio-ulnar incongruence. Further studies are warranted to evaluate the effects of the procedure on joint stability and biomechanics. In the meantime, subtotal coronoidectomy seems especially relevant when the majority of the medial coronoid process (MCP) is damaged (Figure 1).
Should an Ulnar Osteotomy be Performed in all Elbows with FCP?
Transient or persistent radio-ulnar incongruence is now considered as the primary cause for FCP: the radius is shorter than the ulna, creating a high-pressure area over the medial coronoid process, eventually leading to its fragmentation. Ulnar osteotomy may be combined with removal of a FCP if radio-ulnar incongruence is present. The technique actually involves the removal of a short segment of ulna to allow distal migration of the proximal ulna. The osteotomy is performed approximately 25mm distal the elbow and obliqued in a caudo-cranial, proximodistal direction to limit post-operative displacement of the proximal segment. However, a forward tipping and mild medial displacement of the proximal ulna is expected after surgery. This displacement does not appear clinically significant but can be prevented by insertion of an intramedullary pin in the ulna. In a retrospective study of 10 young dogs (less than 10 months), 5 were normal according to their owners 17months after excision of FCP and ulnar osteotomy, while 4 experienced an occasional stiffness and 1intermittent lameness. No crepitus and unchanged range of motion were diagnosed on physical examination in 9 out of 10 dogs (Ness MG 1998). A 93% success rate was also reported after arthroscopic excision of the FCP and proximal ulnar osteotomy, in dogs of all ages (Bardet JF 1997). Further studies are warranted to document the effects of this technique and improve our ability to diagnose radio-ulnar incongruence (see notes on arthroscopic diagnosis of elbow dysplasia).
In spite of research efforts currently directed at improving our ability to diagnose all aspects of elbow dysplasia and optimize the treatment of this condition, recommendations remain largely based on clinical impressions and lack long-term objective evaluation. We currently perform computed tomography and arthroscopy on all elbows suspect of FCP. We recommend arthroscopic excision of FCP, combined with proximal ulnar ostectomy, in dogs with radio-ulnar incongruence. Subtotal excision of the MCP is limited to elbows where the majority of the coronoid process appears damaged.
References
1. Bardet JF, Bureau S: La fragmentation du processus coronoide chez le chien. Prat Med Chir Anim Comp 1996; 31: 451-463.
2. Bardet JF: Arthroscopy of the elbow in dogs. Part II: The cranial portals in the diagnosis and treatment of the lesions of the coronoid process. VCOT 1997; 10: 60-66.
3. Boudrieau RJ, Hohn, Bardet: Osteochondritis Dissecans of the elbow in the dog. J Am Anim Hosp Assoc 1983; 19: 627-635.
4. Boulay JP: Fragmented Medial Coronoid process of the ulna in the dog. Vet Clin North Am 1998; 28: 51-74.
5. Bubenik LJ, Johnson SA, Smith MM, et al.: Evaluation of lameness associated with arthroscopy and arthrotomy of the normal canine cubital joint. Vet Surg 2002; 31: 23-31
6. Morgan JP, Wind A, Davidson A: Hereditary bone and joint diseases in the dog. Schlütersche, 2000.
7. Haudiquet PR, Marcellin-Little DJ, Stebbins ME: Use of the distomedial-proximolateral oblique radiographic view of the elbow joint for examination of the medial coronoid process in dogs. Am J Vet Res 2002; 63: 1000-1005.
8. Lang J, Busato A, Fluckiger M et al: Comparison of two classification protocols in the evaluation of elbow dysplasia in the dog. J Small Anim Pract 1998; 39: 169-174.
9. Mason DR, Schulz KS, Samii VF et al: Sensitivity of radiographic evaluation of radio-ulnar incongruence in the dog in vitro. Vet Surg 2002; 31: 125-132.
10. Meyer-Lindenberg A, Langhann A, Fehr M et al.: Arthrotomy versus arthroscopy in the treatment of fragmented coronoid process of the ulna (FCP) in 421 dogs. VCOT 2003; 16: 204-210.
11. Ness MG: Treatment of fragmented coronoid process in young dogs with proximal ilnar osteotomy. J Small Anim Pract 1998; 39: 15-18.
12. Read RA, Armstrong SJ, Black AP et al.: Relationship between physical signs of elbow dysplasia and radiographic score in growing Rottweilers. J Am Vet Med Assoc 1996; 209.
13. Rovesti GL, Biasibetti M, Schumacher A et al: The use of computed tomography in the diagnostic protocol of the elbow in the dog: 24 joints. VCOT 2002; 15: 35-43.
14. Schwarz PD, Brevard SM, Baker CG: Arthroscopy of the shoulder (OCD) and elbow (MFCP)--thirty consecutive cases each: a comparative study of the early postoperative period. Vet Surg, Proc 7th Annual ACVS symposium; 1993: 21-22.
15. Trostel TC, McLaughlin RM, Pool RR: Canine lameness caused by developmental orthopedic diseases: Fragmented medial coronoid process and united anconeal process. Comp Cont Ed Pract Vet 2003; 25: 112-120.