Horace E. Walcott, DVM, MSPH, MSc
Abstract
A 12.5-kg adult male trumpeter swan (Cygnus buccinator) was presented for necropsy examination in good nutritional status. On the lateral aspect of the right thoraco-abdominal region was an ellipsoidal area of subcutaneous hemorrhage surrounded by a central perforation (gun-shot wound). Two pellets were found in the abdominal blood clots. Toxicology testing indicated 1.5 ppm of lead in the liver. Macroscopic lesions were consistent with of type III gun trauma. Microscopic examination of tissue samples demonstrated disseminated intravascular coagulopathy.
Introduction
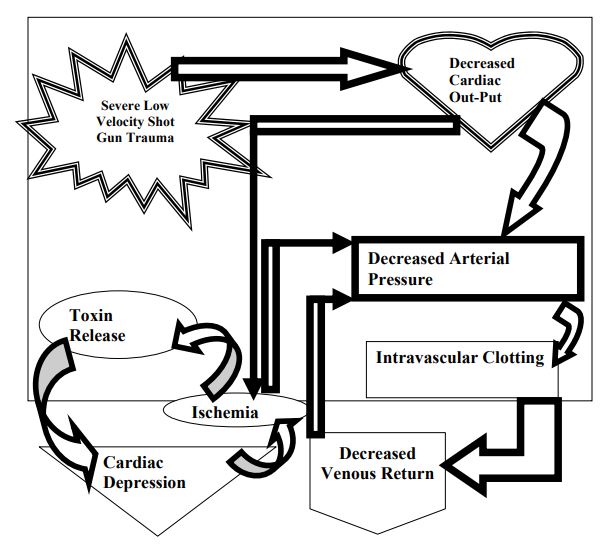
In the mid-western region of the United States, several trumpeter swans (Cygnus buccinator) have been deliberately or accidentally shot during the autumnal migration of Canadian geese (Branta canadensis). Between 1993 and 1994, gunshot contributed to 31% of the mortalities of immature canvasbacks (Aythya valisineria) in inland Louisiana.7 From 1986 to 1992, in the northwestern region of Washington state, illegal shooting and other traumatic factors contributed to 11% and 12% of the total swan mortality, respectively.8 In 1935 excessive hunting and other factors resulted in an Illinois population of less than 100 swans.2 Since then reintroductions from Alaska have replenished the diminishing population. In the cases of accidental shootings, the swans were incorrectly identified as geese. In the autumn of 1994, one swan undergoing intensive care at the Wildlife Ward of the College of Veterinary Medicine, University of Illinois, died of complications associated with gun-shot trauma. The swan was necropsied for macroscopic and microscopic pathologic evaluation. The gross description is reported and the pathologic findings and diagnoses described. Based on human forensic studies, shot gun wounds are classified as type I, type II and type III.1 Type I injuries are sustained at a long range (greater than 7 m) and result in subcutaneous or deep fascia location of pellets. Type II injuries are sustained at a close range of 3 to 7 m and result in the perforation of structures beneath the deep fascia. Type III trauma occurs at point-blank range (less than 3 m). The bullets from a shot gun are usually low velocity. However at a distance of less than 3 m, there is a rapid deceleration of the pellet from an approximate muzzle velocity of 450 m/s.3 Due to the unfavorable ballistic characteristics of a spheroid pellet, the injury to a bird will be severe.8,9 In comparison and contrast with terrestrial mammals, the pathophosiology of multiple trauma due to gun-shots in the aquatic avian species has many similarities and differences, respectively.5,11 The sequela of shock is significant in the pathophysiology of gun-shot trauma in this case and that of avian species in general (Figure 1).1,5,6
Figure 1. Proposed shock pathway in the swan–pathophysiology pathway.f,g
Materials and Methods
'A complete necropsy examination was conducted and tissue samples collected and stored in phosphate buffered formalin. The tissue samples were then processed for histopathology and mounted on slides prior to staining with hemotoxylin and eosin. The stained sections of tissue were microscopically examined.
Results
Gross Description
An adult male trumpeter swan weighing 12.5 kg is presented in good nutritional status. At the distal end of the right ulna and radius, 5–8 cm from the radiocarpal-metacarpal joint, a dark red featherless area (10x4 cm) is present. On the ventral wing surface close to the right proximal phalanx, there is another featherless dark reddened area (4x2 cm). On the lateral aspect of the right thoraco-abdominal region is a 29x13 cm, ellipsoidal area of subcutaneous hemorrhage surrounded by a central perforation (gun-shot wound). The hemorrhagic region extends from the distal sternum to the proximal pelvis on the right side. The segment of the wing with the subcutaneous hemorrhage in the radiocarpal-metacarpal area is slightly mobile and crepitant. Multiple gas bubbles are located on the surface of the abdominal and pectoral muscles with the ellipsoidal area of hemorrhage. Dark red fluid (5–10 ml) is present on the sternal and rib surfaces below the damaged muscles. The proximal and distal segments of the last ribs on the right side are separated from each other 6-8 cm from the sternum. A 4–10 cm diameter circumscribed area is dark red and contains the two fractures. In the right ventro-lateral abdominal region approximately 200 ml of clotted blood extends to the pelvic canal and covers the abdominal viscera. An ovoid, 3x2 cm perforation of 3–4 cm depth is present 5 cm from the greater curvature of the gizzard. Liquid material extends from the proventriculus to the small intestine. Two pellets are found in the abdominal blood clots.
Micromorphologic and Macromorphologic Diagnoses
1. Acute, multiple fractures of the right radius and ulna and two ribs on the right side.
2. Acute, moderate fibrinous thrombosis; systemic vasculature.
3. Acute, multifocal renal infarction.
4. Acute, locally extensive, subscapular hepatic necrosis.
5. Acute, locally extensive, muscle hemorrhage and necrosis; pectoral and abdominal muscles.
6. Focal ulceration; right ventral wing.
7. Mild to moderate, subacute pericholangitis.
Conclusion
The cause of death was most likely due to shock and disseminated intravascular coagulation (DIC) secondary to trauma from gun shots. The contribution of bacteria isolated from the pectoral muscle wound is insignificant.3-6
Discussion
The lesions in the swan are consistent with thoracic and abdominal trauma due to gun shots.9,10,12 The multiple fractures and radiologic data demonstrating the presence of radio-opaque pellets in the thorax and abdomen corroborated the toxicologic data, which indicated lead in liver tissue. The micro-pathologic findings are consistent with DIC.
Table 1. Summary of macromorphologic diagnoses
|
Organ system
|
Diagnosis
|
|
Abdomen
|
Acute, moderate hemoperitoneum
|
|
Musculoskeletal
|
Acute, locally extensive, necrohemorrhagic myositis of the pectoral and abdominal muscles (gun shot).
Acute, multiple compound fractures of the radius and ulna and the last two right ribs (gun shot).
|
Table 2. Summary of microscopic lesions
|
Organ system
|
Lesion
|
|
Rostral and
mid-cerebrum
|
Fibrin thrombi in the intra-cerebral and leptomeningeal vessels.
|
|
Lung
|
Locally extensive area of hemorrhage, edema, and mild congestion.
|
|
Liver
|
Coalescing subcapsular areas of necrosis with adjacent areas of bile ductular proliferation with moderate infiltrates of mononuclear cells and heterophils.
Hemosiderophages are present in the areas of necrosis and fibrosis present in the portal triads.
Attached to the overlaying serosal surface is an eosinophilic material containing erythrocytes.
Toxicology findings. Liver 1.5 ppm lead. The lead level is higher than background concentration and not suggestive of lead toxicosis.
|
|
Kidney
|
Linear areas of tubular degeneration and congestion extending from the subscapsular area into the cortex.
Fibrin thrombi are present in some associated vessels.
|
|
Skin
|
Segmental loss of the epidermis with a thick layer of eosinophilic material mixed with inflammatory cells and bacterial colonies.
In the subjacentarea there is hemorrhage and edema and an arteriole containing a thrombus.
|
Acknowledgments
The histopathology was performed by Dr. Wanda Haschek-Hock of the Department of Pathology, University of Illinois, College of Veterinary Medicine. My fellowship in Toxicological Pathology was funded by a grant from the Pfizer Pharmaceutical Corporation.
Literature Cited
1. Anderson, J. R. 1980. Disturbances in blood and body fluids. In: Anderson, J. R. (ed.). Muir’s Textbook of Pathology. Edward Arnold, London. 260–266.
2. Cooke, A. 1994. Trumpeter Swan Dies at UI Clinic. Champaign-Urbana News-Gazette, Wednesday, November 30, A4.
3. De Muth, W. E. 1971. The mechanism of shot gun wounds. J. Trauma. 11: 219.
4. Graham, D. L. 1984. An update on selected pet bird virus infection. Proc. Intern. Conf. Avian Med. (Assoc. Avian Vet.) 267–280.
5. Guyton, A. C., and J. E. Hall. 1994. Circulatory shock and physiology of its treatment. In: Textbook of Medical Physiology. W. B. Saunders Co., London, England. Pp. 285-294.
6. Green, R. A., and J. S. Thomas. 1995. Homeostatic disorders: coagulopathies and thrombosis. In: Ettinger,
7. S. J., and E. C. Feldman (eds.). Textbook of Veterinary Internal Medicine, 4th ed. W. B. Saunders Co., 1946–1963
8. Hohman, W. L. 1995. Winter survival of immature canvasbacks in inland Louisiana. J. Wildl. Manag. 59: 384–391.
9. Lagerquist, J. E., M. Davison, and W. J. Foreyt. 1994. Lead poisoning and other mortalities in trumpeter swans (Cygnus buccinator) and tundra swans (C. columbianus). J. Wildl. Dis. 30: 60–64.
10. Martin, D. U. B. 1971. The management of shotgun wounds. J. Trauma. 11: 522.
11. McKenzie, H. J., J. A. Coil, and R. N. Ankney. 1995. Experimental thoracoabdomonial airgun wounds in porcine model. Trauma. 39: 1164–1167.
12. Powers, V. L. 2000. Avian Hemostasis. In: Fudge, A. M, (ed.). Laboratory Medicine–Avian and Exotic Pets. Elsevier Health Sciences, New York, New York, Pp. 3–546.
13. Zuidema, G. D., and W. F. Ballinger II. 1979. Abdominal Injuries. In: Zuidema, G. D., R. B. Rutherford, and W. F. Ballinger II (eds.). The Management of Trauma, 3rd ed. W. B. Saunders Co., London, England. 431–481, 541.