David M. Vail, DVM, DACVIM(Oncology)
The majority of neoplastic disorders presenting to the practitioner are manageable in the practice setting and advances in cancer chemotherapeutics are realised virtually every year. More and more clients are searching (often on the Internet) for high-quality care for their companions with cancer.
These points in combination with the high incidence rate of neoplasia in our companion animal population make an understanding of the principles of chemotherapy a benefit to the practitioner and the client alike.
General Principles
A therapeutic strategy should be clearly defined for each patient based on the identified histology and clinical stage of the disease. The full cooperation of the owner is essential: all aspects of the plan must be clearly explained, ideally through the use of handouts which the owners can read and consult as needed. The first and foremost goal of cancer therapy is to sustain or improve the animal's quality of life. The secondary goal is to stabilise, decrease, or eliminate the neoplastic process. There exist five potential roles for chemotherapy:
 Induction therapy for advanced disease
Induction therapy for advanced disease
As an adjunct to local therapy
Primary or neoadjuvant therapy (i.e., prior to surgical excision)
Instillation into sanctuaries
Palliation
Basic Cell Kinetics
Tumour growth is best described by the Gompertz growth curve (Figure 1). Note that our diagnostic abilities are such that clinical and radiographic diagnosis occurs near the end of the logarithmic growth phase of the cancer (i.e., the point where chemotherapy is most effective), often necessitating combined modalities of therapy (e.g., adjuvant surgical or radiotherapeutic cytoreduction). As well, the larger the tumour volume, the more likely tumour clones capable of drug resistance and metastasis will have arisen.
| Figure 1. Gompertz growth curve. | 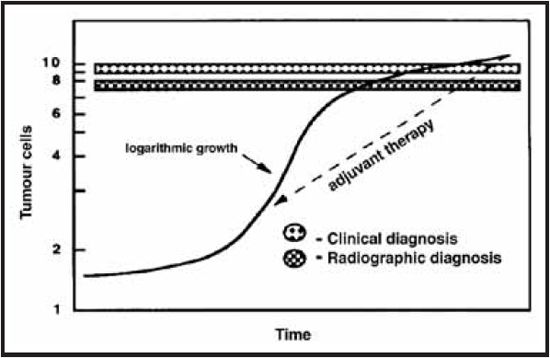
|
|
| |
Drug Choice and Dosage
Certain chemotherapeutics act only on specific portions of the cell cycle and are termed 'cell cycle specific agents' (e.g., vincristine acts during the formation of the mitotic spindle). Others affect the cell cycle in a variety of locations and are known as 'cell cycle non-specific' (e.g., alkylating agents like cyclophosphamide). Combination drug protocols are theoretically most effective when the drugs used in combination act at different stages of the cell cycle. When choosing a combination protocol, several key elements should be considered. Only choose drugs proven to have efficacy when used alone; select each drug on the basis of toxicity (i.e., try to avoid drugs with overlapping toxicities), and ideally, combine drugs that have different mechanisms of action. The determination of chemotherapeutic drug dosages should be based on several generalities. The ultimate objective is to elicit maximal anti-tumour effect concomitant with minimal host toxicity. The phenomenon of tumour drug resistance is the leading cause of drug failure. Tumour cells have an unstable genetic makeup, which allows resistant mutations to occur at a relatively regular rate; the larger the tumour volume, the more likely such a mutation is present in one of the tumour clones. In general, when a tumour gains resistance to a drug, it gains resistance to other drugs, which act by similar mechanisms. Also, multiple drug resistance (MDR, pleotrophic drug resistance) may develop that allows a tumour to be resistant to a wide variety of drug types.
Clinical End-Points
Once a patient is started on chemotherapy, there must be a clear method of evaluating the tumour response so that future treatment decisions can be made. All tumours should be measured prior to treatment. See introductory lecture notes "General Introduction to Veterinary Oncology" for clinical end-points.
Drug Handling and Safety
Most chemotherapeutics are known to be carcinogenic and teratogenic in their own right. It is prudent that the clinician, caregiver and any technical staff who may come in contact with these agents be forewarned as to their potential toxicity. In the ideal situation, all solutions would be prepared in a fume hood by a clinical pharmacist. In the practice setting, common sense and regionally mandated guidelines should be the rule. Staff who are pregnant or are trying to become so should avoid handling these agents. Latex gloves and goggles should be worn during the preparation and handling of all solutions. Masks should be worn during solution preparations and spill sheets (e.g., disposable diapers) should be used in the area of preparation. Luer locks should be used to protect against inadvertent spray. After drug handling, the preparation area as well as the operator's hands should be washed thoroughly. With drugs primarily cleared by urinary excretion, handle urine with appropriate care. Check local ordinances with regard to disposal of contaminated items.
Caregiver Concerns Regarding the Use of Chemotherapy in Their Companions
My Great Aunt Harriet had chemo, and she felt miserable all the time--I'd never do that to my pet!
The drugs we use to treat cancer in animals are the same drugs that humans receive; however, we give considerably lower doses and don't use as many at the same time to minimise the risk of adverse effects. With most chemotherapy protocols in common use, less than a quarter of patients experience unpleasant side effects (usually transient), and 5% or less experience a severe side effect. The rare adverse event necessitating hospitalisation can usually be resolved in 24-72 hours. The likelihood of a chemotherapy-related fatality is less than 1 in 200. Should unpleasant side effects occur, doses can be reduced, drugs can be substituted, or additional medications dispensed to minimise the likelihood of further adverse effects. These changes are effective 90% of the time. The author's interactive session at this conference will address adverse events.
Ok, suppose my dog is the unfortunate one that has a side effect? What kind of side effects are we likely to see?
This varies by agent, but in general the most common side effect is something related to the gastrointestinal tract: perhaps a few days of decreased appetite, mild nausea or vomiting, or loose stool. By way of comparison, it's usually not too different from what you might see if a dog got into the garbage or ate something they shouldn't have in the back yard. They might need to eat some bland food for a few days or take some anti-nausea or anti-diarrhoea pills at home. Usually this doesn't persist for more than 2-3 days. Some dogs develop a lowering of the white blood cell count. We check this frequently, and most of the time it is not low enough to be dangerous. In some cases, oral antibiotics may be needed, or a treatment might need to be delayed for a few days.
I don't want Fluffy to go bald! Is it true that certain dog breeds (the so-called non-shedding breeds) can lose some hair from chemotherapy?
It is rarely complete. Most breeds experience little or no hair loss, although the owners will find more hair around the house. Hair loss from chemotherapy is non-itchy and non-painful; it is a purely cosmetic change. Hair that is lost will typically begin to regrow following the completion of therapy. Cats may lose whiskers and the long, stiff 'guard hairs' of their coat.
I don't want Spike's last weeks/months/ years to be in and out of the hospital, like they were with Uncle Mac when he had cancer, is this possible?
Almost all veterinary chemotherapy treatments are done in an outpatient setting, and most involve quick injections rather than prolonged infusions.
I don't want my family/guests/house/other pets to be contaminated, is this a common problem?
Urine and faeces pose a minimal risk to owners--few drugs are excreted for longer than 48 hours. Common sense (i.e., wear gloves when handling urine or faeces) is usually sufficient. Accidents in the house during this period should be cleaned using a dilute bleach solution and the excreta flushed down the toilet. Normal daily interactions (grooming, playing, petting, handling food and water bowls) pose no real risk. It is important that owners are instructed to wear gloves when handling oral medications, and that pills not be crushed or split, or capsules opened.
But what about Muffy's age? Isn't she too old for treatment?
Age is not a disease! Most of the patients we treat with cancer are older pets. Statistics regarding effectiveness, survival and tolerability of cancer therapy are usually generated in a population of older patients. Far more important than chronological age are general health (e.g., cardiovascular, renal) and performance status (e.g., how are they feeling?).
So what are our choices? We either do chemo or put him to sleep?
Chemotherapy (and cancer therapy in general) is generally not an 'all-or-nothing' proposition. For many tumour types, a spectrum of treatment options may be available depending on owner availability, finances, willingness to tolerate side effects, etc. All have different costs, risks of side effects and numbers of trips required and varying degrees of efficacy.
Breed Predisposition to Adverse Effects of Chemotherapy
Certain breeds, in particular collies, are known to be at risk for toxicity from chemotherapeutics. These breeds have a high frequency of a pharmacogenetic mutation of the MDR1allele (Figure 2.) If a dog is homozygous for the mutant allele, they will be affected and at risk; if they are heterozygous for the mutant allele, they are a carrier.
Figure 2. Frequency of the MDR1 pharmacogenetic mutation in breeds from three geographic locations (HT = heterozygous (carrier); HO = homozygous (affected)).
|
Breed |
US |
France |
Australia |
|
HT |
HO |
HT |
HO |
HT |
HO |
|
Australian Shepherd Dog |
29.8 |
1.7 |
- |
- |
42.8 |
21.4 |
|
Australian Shepherd Dog (mini) |
44.6 |
3.6 |
- |
- |
|
Border Collie |
46.8 |
31.2 |
32 |
48 |
64 |
24 |
|
Long-haired Whippet |
51.7 |
15.7 |
- |
- |
- |
- |
|
Shetland Sheepdog |
14.7 |
1.1 |
- |
- |
42.8 |
0 |
References
1. Chun R, Garrett LD, Vail DM. Cancer chemotherapy. In: Withrow, SW; Vail, DM. eds. Small animal clinical oncology (fourth edition). St. Louis: Saunders/Elsevier, 2007; 163-192.