Professor, Department of Clinical Veterinary Science, Royal Veterinary College, Hawkshead Campus
North Mymms, Hertfordshire, UK
Introduction
Adverse reactions to food (AFR) cover a spectrum of conditions including dietary indiscretion and food aversion as well as food allergy and intolerance (Figure 1). This review will be restricted to AFR recognised as differential diagnoses for non-seasonal pruritic diseases of the skin in dogs and which may also cause gastrointestinal, respiratory, urinary tract (cystitis) and neurological problems.1,2 These reactions are thought to include immunological (food allergies) and non-immunological (food intolerances or non-allergic food hypersensitivities) causes, although differentiation between these causes is rarely made in veterinary clinical practice.
The prevalence of canine AFR remains controversial.5,6,7 Within referral populations, studies have estimated AFR to be responsible for 5% of canine dermatoses8 and 10-15% of canine allergic dermatoses.9,10 More recently, AFR has been described as the sole cause of skin disease in 20-35% of dogs with non-seasonal pruritus.6,7,11
| Figure 1. The spectrum of adverse reactions to food. | 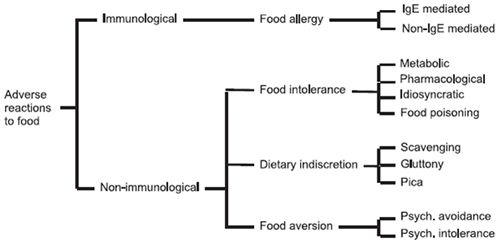
|
|
| |
Clinical Signs in AFR
Signs are nearly always non-seasonal but can be related to seasonal factors e.g., concurrent atopy or flea allergy, ectoparasites, or seasonal variation in diet. Signs may be related to skin and/or to the gastrointestinal tract. In addition, cystitis, respiratory or neurological signs have been reported.1,2
Cutaneous signs normally include pruritus and erythema, which may affect any part of the skin. There is often otitis externa and, in severe cases, otitis media. Secondary pyoderma, pyotraumatic dermatitis, microbial overgrowth and signs related to chronic pruritus (hair loss, hyperpigmentation, lichenification, excoriation and ulceration) commonly occur.11 Often there is scaling and poor coat. Lesions can be restricted to parts of the skin and, rarely, may be unilateral. Cutaneous signs may mimic those of other pruritic dermatoses including ectoparasitic infestations, such as scabies and cheyletiellosis, and atopy and flea allergy, diseases which may also occur concurrently. However, perineal pruritus may be a pointer towards AFR.
Gastrointestinal signs occur with increased frequency in pruritic dogs with AFR.11 Signs may include increased defecation frequency, soft faeces, intermittent diarrhoea and flatulence. However, in some dogs with AFR resulting in cutaneous disease, gastrointestinal signs are absent.
Diagnosis of Adverse Reactions to Food
Clinical signs of pruritic disease consistent with allergy should always raise suspicion of AFR, particularly with concurrent gastrointestinal signs and/or perineal pruritus. However, diagnosis cannot be made on the basis of the clinical presentation as AFR can mimic other pruritic diseases.
Several procedures have been described for the diagnosis of AFR. These include serology, cutaneous tests (intradermal, patch), gastroscopic provocation and intestinal permeability tests. However, these procedures have not been validated12-19 and dietary elimination trials followed by dietary provocation remain the procedure of choice.
Diets for diagnostic trials can either be home-prepared foods or commercial products. Home-prepared diets are traditionally recommended as the "gold standard" for diagnosis of canine AFR as they can be tailored to each dog's dietary history individually avoiding foods to which the animal has already been exposed.20,21 However, such diets are labour-intensive for owners and ingredients novel to the dog may not be readily available. They are also not adequate for maintenance after diagnosis or for diagnosis in young, growing dogs.22,23
Commercial diets using limited and less commonly fed ingredients have been shown to be inferior to home-cooked diets in most comparative studies in diagnosis of AFR.11,24,25,26 Furthermore, individual dogs have been described that tolerate home-prepared ingredients but not their commercially prepared versions, raising concerns over processing additives.1,25,27,28 However, allergenic food additives have not been characterised in dog foods.28
More recently, hydrolysed veterinary diets have been introduced for diagnosis of canine AFR. During hydrolysis, protein sources (chicken, poultry liver, casein, soy) are broken down to polypeptides, changing and reducing their allergenic properties. Two clinical investigations into possible AFR in pruritic dogs, one using a chicken hydrolysate diet,10 the other a soy-based hydrolysate,7 reported similar frequencies of AFR as in a study with home-prepared diets.6 A subsequent retrospective study examining home-cooked diets and the chicken hydrolysate diet in a referral centre suggested that were equally useful in the diagnosis of canine AFR.29
The clinical approach to diagnosis of AFR in pruritic dogs should involve:
1. Selection of dogs with non-seasonal pruritus or a history suggestive of AFR.
2. Careful recording of clinical signs and owners' observations relating to pruritus, lesions and gastrointestinal signs.
3. Tests for ectoparasitic infestation. These may include serology for sarcoptic mange and examination of skin scrapings, coat brushings of hair pluck samples.
4. Flea control, on the dog and in the environment, and trial therapy to eliminate ectoparasitic infestation and remove flea challenge.
5. Treatment of pyoderma or microbial overgrowth with systemic antibiotics and/or topical therapy until all lesions are eliminated.
6. Maintenance of a rigorous food-restriction trial for 6 to 8 weeks. In addition to the chosen diet, only water may be given to drink. Home-cooked or limited ingredient commercial diets are selected based on the dietary history of the dog; a protein and a carbohydrate source seldom or never fed previously are selected. With hydrolysed diets, palatability may be important. If dry, moistening the diet may improve palatability; generally dogs adapt to the diet after a few days.
7. Maintenance of contact with the owner to monitor the results and ensure that all treatments and the diet are properly instituted.
8. Dietary challenge, after the trial, with the foods, drinks and treats formerly given. Some owners may refuse to challenge the dog once a good response has been obtained and wish to continue with the restriction diet. With home-cooked diet it will be necessary to provide supplements to make it balanced, or persuade the owner to use an equivalent commercial diet. Remember that you have not yet proved that this problem is AFR; beware of seasonal or other factors which may have led to the animal's improvement.
9. Evaluation and recording of changes in clinical signs and owners' observations in response to treatment, the restriction diet and dietary challenge.
10. If there is complete response to diet and signs recur on challenge, AFR can be diagnosed.
11. Where there has been partial response and signs recur on challenge, AFR concurrent with other pruritic disease can be diagnosed. Because of the rule-outs, this disease is likely to be atopy.
Management of Dogs with Adverse Reactions to Food
Diagnosis of AFR should be presented to the owner as a "good news" story. Now the disease can be controlled only by dietary management. Often the animal will show improvements associated with improved gastrointestinal function which will please the owner, such as elimination of flatulence, improved appetite, reduced scaling, a glossier coat, more energy. It is useful to draw such changes to the attention of the owner.
It is important to make the owner feel responsible and part of the "team" dealing with the problem as dietary control will need to be maintained for the rest of the dog's life. Keeping in regular contact is essential as occasionally the diet will be broken and pruritus, pyoderma and other signs of the disease will recur and need to be treated. The owner may also begin to experiment with forbidden treats and may not appreciate that signs of reactivity can take several days to appear. In addition, other pruritic diseases or allergies may develop and the dog may become sensitive to additional dietary components and may need to be worked up and tested again.
References
1. Rosser EJ. Diagnosis of food allergy in dogs. Journal of the American Veterinary Medical Association 1993 203 259-262.
2. Guilford, W.G. (1996) Adverse reactions to food. In: Guilford WG. et al. eds. Strombeck's Small Animal Gastroenterology. 3rd edn. Philadelphia: W.B.Saunders 1996 436-450.
3. ?
4. ?
5. Walton GS. Skin responses in the dog and cat to ingested allergens. Observations on 100 confirmed cases. Veterinary Record 1967 81 709-713.
6. Chesney CJ. Food sensitivity in the dog: a quantitative study. Journal of Small Animal Practice 2002 43 203-207.
7. Biourge VC, Fontaine J, Vroom MW. Diagnosis of adverse reactions to food in dogs: efficacy of a soy-isolate hydrolysate-based diet. Journal of Nutrition 2004 134 2062S-2064S.
8. Willemse, T. Adverse reactions to diet: an update on clinical manifestations. Royal Canin Symposium on Adverse Reaction to Food, 5th World Congress of Veterinary Dermatology, Vienna, August 25th 2004, pp. 8-9.
9. Ackerman L. Food hypersensitivity: a rare, but manageable disorder. Veterinary Medicine 1988 83 1142-1148.
10. Carlotti DN, Remy I, Prost C. Food allergy in dogs and cats. A review and report of 43 cases. Veterinary Dermatology 1990 1 55-62.
11. Loeffler A, Lloyd DH, Bond R. et al. Dietary trials with a commercial chicken hydrolysate diet in 63 pruritic dogs. Veterinary Record 2004 154 519-522.
12. Jeffers JG, Shanley KJ, Meyer EK. Diagnostic testing of dogs for food hypersensitivity. Journal of the American Veterinary Medical Association 1991 198 245-250.
13. Kunkle G, Horner S. Validity of skin testing for diagnosis of food allergy in dogs. Journal of the American Veterinary Medical Association 1992 200 677-680.
14. Elwood CM, Rutgers HC, Batt RM. Gastroscopic food sensitivity testing in 17 dogs. Journal of Small Animal Practice 1994 35, 199-203.
15. Mueller R, Tsohalis J. Evaluation of serum allergen-specific IgE for the diagnosis of food adverse reactions in the dog. Veterinary Dermatology 1998 9 167-171.
16. Foster AP, Knowles TG, Hotston Moore A et al. Serum IgE and IgG responses to food antigens in normal and atopic dogs, and dogs with gastrointestinal disease. Veterinary Immunology and Immunopathology 2003 92 113-124.
17. Jackson HA, Jackson MW, Coblentz L, Hammerberg B. Evaluation of the clinical and allergen specific serum immunoglobulin E responses to oral challenge with cornstarch, corn, soy and a soy hydrolysate diet in dogs with spontaneous food allergy. Veterinary Dermatology 2003 14 181-187.
18. Halliwell REW, Gordon C, Horvath C et al. IgE and IgG antibodies to food antigens in sera from normal dogs, atopic dogs and dogs with adverse food reactions. Veterinary Dermatology 2004 15 (Suppl.1) 2.
19. Ishida R, Masuda K, Kurata K et al. Lymphocyte blastogenic responses to inciting food allergens in dogs with food hypersensitivity. Journal of Internal Veterinary Medicine 2004 18 25-30.
20. Reedy, LM., Miller, WH. & Willemse, T. (1997) Food hypersensitivity. In: Reedy LM. Et al. eds. Allergic skin diseases of dogs and cats. 2nd edn. London: W.B.Sauders 1997 173-188.
21. Scott DW, Miller WH, Griffin CE. Skin immune system and allergic skin diseases. In: Scott DW, Miller WH, Griffin CE. eds. Muller & Kirk's Small Animal Dermatology 6th edn. Philadelphia: W.B. Saunders 2001 543-666.
22. Roudebush P, Cowell CS. Results of a hypoallergenic diet survey of veterinarians in North America with a nutritional evaluation of homemade diet prescriptions. Veterinary Dermatology 1992 3 23-28.
23. Streiff EL, Zwischenberger B, Butterwick RF et al. A comparison of the nutritional adequacy of home-prepared and commercial diets for dogs. Journal of Nutrition 2002 132 1698S-1700S.
24. Tapp T, Griffin C, Rosenkrantz W. et al. Comparison of a commercial limited-antigen diet versus home-prepared diets in the diagnosis of canine adverse food reaction. Veterinary Therapeutics 2002 3 244-251.
25. Roudebush P, Schick RO. Evaluation of a commercial canned lamb and rice diet for the management of adverse reactions to food in dogs. Veterinary Dermatology 1994 5 63-67.
26. Leistra MHG, Markwell PJ, Willemse T. Evaluation of selected-protein-source diets for management of dogs with adverse reactions to foods. Journal of the American Veterinary Medical Association 2001 219 1411-1414.
27. Rutgers HC, Batt RM, Hall J. et al. Intestinal permeability testing in dogs with diet-responsive intestinal disease. Journal of Small Animal Practice 1995 36 295-301.
28. Hannuksela M, Haahtela T. Hypersensitivity reactions to food additives. Allergy 1987 42 561-575.
29. Loeffler, A. Soares-Magalhaes, R., Bond, R. et al. A retrospective analysis of case series of home-prepared and chicken hydrolysate diets in the diagnosis of adverse food reactions in 181 pruritic dogs. Veterinary Dermatology 2006. In press.