D. Smeak
Veterinary Clinical Sciences, Colorado State University, Fort Collins, CO, USA
Gastropexy for treatment of gastric dilatation volvulus (GDV) is often performed as an emergency procedure, therefore, an ideal method for gastropexy should be quick, safe and easy to perform. This article describes an incisional gastropexy technique designed to be readily performed by a surgeon without assistance for treatment of acute GDV and to prevent this condition. Like other successful permanent gastropexy techniques, this method apposes incised surfaces of the right abdominal wall and pyloric antrum. Illustrated technical details are included that allow the surgeon to readily create these incised surfaces while avoiding potential complications such as inadvertent perforation of the gastric mucosa or diaphragm. In addition, standard gastropexy incision sites are described and shown to help prevent gastric malpositioning or outflow obstruction following surgery. Technique with the animal in dorsal recumbency, aseptically prepare the ventral abdomen. The surgeon stands on the left side of the patient for the best exposure to the gastropexy site; the figures in this article are viewed from this perspective. Create a linea alba incision from the xiphoid to umbilicus. This incision should be long enough to perform the gastropexy and allow complete abdominal exploration. If more cranial exposure is needed in deep-chested dogs, continue to cut the linea incision (cranial but superficial to the xiphoid cartilage) with Mayo scissors. Remove the falciform fat to access the abdominal wall gastropexy site. Grasp the right side of the cranial abdominal wall incision, evert and roll the wall to allow palpation of the chondral aspect of rib twelve. The twelfth rib can be identified by palpating its cartilaginous margin that ends several centimetres caudal to the xiphoid cartilage. The reader should note that there are individual breed differences in the location of the chondral aspect of ribs eleven and twelve. The eleventh rib can be used alternatively if the cartilaginous end of this rib is located several centimetres caudal to the xiphoid (Fig. 1). Remove the falciform fat and isolate the twelfth rib with your thumb and index finger and pull the rib away from deeper structures (Fig. 2). Place two towel clamps around the isolated rib approximately five to six centimetres apart from one another (Fig. 3). The cranial clamp should be positioned at the end of the twelfth rib approximately 5 centimetres caudal to the xiphoid (Fig. 1). Elevation of this rib by the towel clamps helps stabilize the rib and retracts it away from the diaphragm. In one stroke, directly incise over the twelfth rib with a scalpel blade between the towel clamps (Fig. 3). The abdominal wall incision is about midway between the dorsal and ventral aspects of the right abdominal wall (Fig. 4). The stomach incision site is made midway between the pylorus and base of the antrum (Fig. 5). Orient the stomach incision parallel to the long axis of antrum, and midway between lesser and greater curvatures to avoid damage to stomach vasculature. Thoroughly wipe and dry your left thumb and index finger with a dry sponge. Carefully wipe the surface of the proposed antral gastropexy site (Fig. 6). Pinch about 4 centimetres of the antral site (full-thickness) between the thumb and index finger (held parallel to the long axis of the antrum) (Fig. 6). Lift the pinched stomach wall until the mucosa distinctly slips out from between the fingers.
What remains grasped after this manoeuvre is just the serosa and muscular layer of the stomach wall. With Metzenbaum scissors, create a partial thickness gastric antral incision by cutting to the base of the pinched wall towards the tips of the fingers (Fig. 7). Since the gastric mucosa has been squeezed away from the pinched wall, no perforation into the stomach is possible and only the seromuscular layer is incised (Figs. 7 and 8). The stomach incision should be 3–4 centimetres in length.
Bring the stomach wound in apposition to the rib incision so that the pylorus is pointing in a craniodorsal direction. Fasten stay sutures to both ends of the incisions thorough the seromuscular stomach layer and transverse abdominal muscle. (Fig. 9) Use 2-0, prolonged absorbable or nonabsorbable monofilament suture material (i.e., polydioxanone) on a taper needle. When stay-sutures are placed and tied, the incised edges of the stomach and abdominal wall are brought in apposition so the edges are easy to suture (Fig. 9). Leave the needles attached to the stay sutures so that they can be used to appose the incision edges for the gastropexy. With the cranial stay suture needle, begin suturing the caudal edge (greater curvature side) of the incised stomach wall to the dorsal edge of the abdominal wall incision (the two muscle edges between stomach mucosa and rib) with a simple continuous suture pattern (Fig. 10). At least 3–4 mm bites of tissue should be included on either side of the suture line. Avoid entering the stomach lumen with the needle if possible. The first suture line is ended and tied to the knot ears of the stay suture at the other end of the incision. Using the needle from the caudal stay suture, appose the remaining (lesser curvature side) free edge of the stomach incision to the ventral part of the abdominal wall incision using the same suture pattern (Fig. 11). Tie this suture line to the knot ears of the cranial stay suture knot. After both suture lines are completed, both incision edges of the stomach and abdominal wall are firmly apposed (Fig. 12). Close the celiotomy incision in a routine fashion.
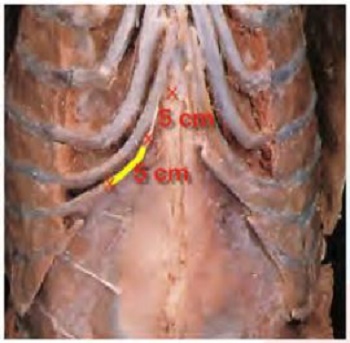
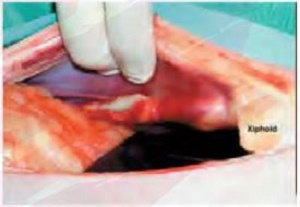
Figure 1
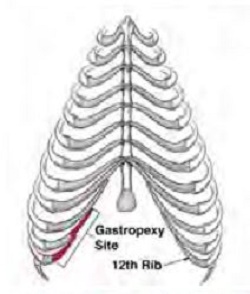
The gastropexy site over the 11th or 12th rib is highlighted in red (top). On a ventral thoracic view in a cadaver, the abdominal wall incision site is 5 cm caudal to the tip of the xiphoid cartilage and about 5 cm in length (yellow line)
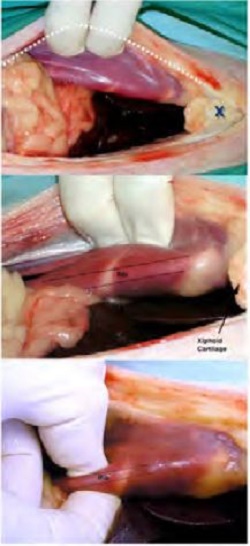
Figure 2
The falciform fat is removed from the celiotomy incision (dotted line) and the full-thickness right abdominal wall is pulled forcibly to the right to expose the rib margin seen under the peritoneal surface (top) “X” marks the cranial part of the celiotomy incision, the base of the xiphoid cartilage (bottom 2 images). While holding the abdominal wall to the right, the 12th rib is palpitated and fixed between the surgeon’s index finger and thumb.
Figure 3
Towel clamps are placed through the transverse abdominal muscle and around the isolated pinched rib. Transverse abdominal muscle is incised directly over the isolated rib, which is held up and exposed by towel clamps.
Figure 4

Towel clamps are removed (just for illustration purposes after the incision is complete to show the location of the abdominal incision when it is completed. Note the correct site of the 5 cm incision is about 5 cm caudal to the xiphoid cartilage. In a real clinical case, the towel clamps are left in place to hold and expose the incision site until the gastropexy is completely sutured.
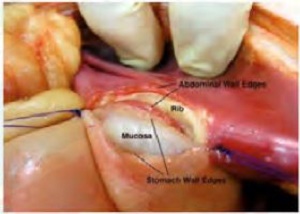
Figure 5
The correct antral site for the stomach wall incision (oval black mark). This site is midway between the lesser and greater curvatures, and midway between the pylorus and antral-body line (black line).
Figure 6

After the surface and fingers have been wiped dry (top), the full-thickness stomach wall is pinched between the thumb and index finger at the correct antral site denoted in Figure 5 (bottom). The area is pinched and lifted such that the mucosa is felt to slip out away from the grasped (isolated) serosal and muscular layers.
Figure 7

The mound of stomach wall held with the index finger and thumb is cut just adjacent to the fingers (top) with Metzenbaum scissors. Since the mucosa has slipped out of the grasped stomach wall, the cut simply cannot penetrate the stomach lumen (middle). Thumb and index fingers are placed at the “X” marks. The incision is oriented as depicted as the purple line between the “X” marks. Completed incision (bottom).
Figure 8

After cutting the serosal and muscular layers, the intact whitish bulging mucosa is exposed. The incised stomach wall edges are now ready to be sutured to the abdominal wall incision margins.
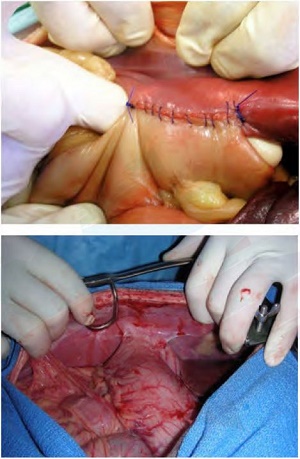
Figure 9

Position the pylorus in a craniodorsal direction and knot preplaced stay sutured at the opposite sides of the incision, holding the stomach and abdominal wall incisions in apposition.
Figure 10
The “deep” (greater curvature side) edge of the stomach incision and dorsal edge of the abdominal wall incision are sutured together with continuous 2-0 prolonged absorbable monofilament suture.
Figure 11

The ventral portion of the abdominal wall incision is opposed to the adjacent stomach wall incision.
Figure 12
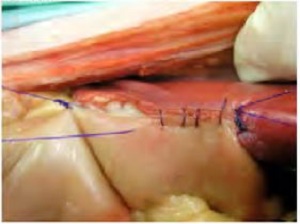
Completed gastropexy closure (top). Two continuous suture lines hold the stomach to the abdominal wall securely (bottom). “Smeakopexy” site one-year after treatment for acute GDV in a German shepherd dog.
Figure 13