Theresa W. Fossum, DVM, MS, PhD, DACVS
TRACHEAL TRAUMA
Tracheal trauma is uncommon but may occur secondary to bite wounds, gunshot wounds, endotracheal intubation, or other injury. Small lacerations will often heal on their own with conservative therapy; however, the sequelae of tracheal trauma may be stricture or severe acute respiratory distress necessitating temporary tracheostomy or tracheal resection and anastomosis.
Temporary Tracheostomy
Tracheostomy allows air to enter the trachea distal to the nose, mouth, nasopharynx, and larynx. A tracheotomy is performed, and either a tube is inserted (temporary tracheostomy) or a stoma is created (permanent tracheostomy) to facilitate airflow. A nonreactive tube that is no larger than one half the size of the trachea should be selected. Cuffed or cannulated autoclavable silicone, silver, or nylon tubes are recommended. Polyvinyl chloride and red rubber tubes are irritating and should be avoided. If the animal is being placed on a respirator, a cuffed tube is necessary.
| 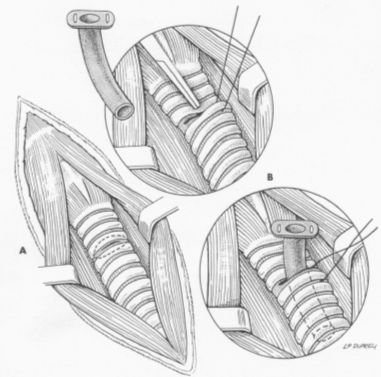
Figure 1. From: Fossum, TW: Small Animal Surgery, Mosby, 2002 |
|
| |
Temporary tracheostomy is most commonly performed to provide an alternate airflow route during surgery or as an emergency procedure in severely dyspneic patients. Tube tracheostomies are usually maintained for a short time. Make a ventral midline incision from the cricoid cartilage extending 2 to 3 cm caudally. Separate the sternohyoid muscles and make a horizontal (transverse) tracheotomy through the annular ligament between the third and fourth or fourth and fifth tracheal cartilages. Do not extend the incision around more than half the circumference of the trachea. Alternatively, make a vertical tracheotomy across the ventral midline of cartilages 3 through 5. Suction blood and mucus from the lumen, widen the incision, and insert the tracheostomy tube. Facilitate tube placement by encircling a cartilage distal or lateral to the incision with a long stay suture. Place tension on this suture to open the incision. Alternately, open a hemostat in the incision or depress the cartilages cranial to the horizontal incision. Resect a small ellipse of cartilage if tube insertion is difficult. Appose the sternohyoid muscles, subcutaneous tissue, and skin cranial and caudal to the tube. Secure the tube by suturing it to the skin or tying it to gauze that is tied around the neck (see Figure 1).
Tracheal Resection/Anastomosis
Removal of a tracheal segment may be necessary to treat tracheal tumors, stenosis, or trauma. Depending on the degree of tracheal elasticity and tension, approximately 20% to 60% of the trachea may be resected and direct anastomosis achieved. The split cartilage technique is preferred because it is easier to perform and results in more precise anatomic alignment with less luminal stenosis than many other techniques. Diseased trachea exceeding the limits of resection and anastomosis may be managed with permanent tracheostomy, intraluminal silicone tubes, grafts, or prostheses with variable success (see Figure 2).
| 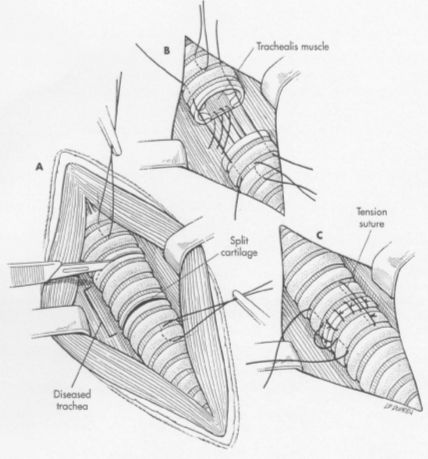
Figure 2. From: Fossum, TW: Small Animal Surgery, Mosby, 2002 |
|
| |
Expose the involved trachea through a ventral cervical, midline, lateral thoracotomy, or median sternotomy approach. Mobilize only enough trachea to allow anastomosis without tension. Preserve as much of the segmental blood and nerve supply to the trachea as possible. Place stay sutures around cartilages cranial and caudal to the resection sites prior to transecting the trachea. Resect the diseased trachea by splitting a healthy cartilage circumferentially at each end or incising annular ligaments adjacent to the intact cartilages. Use a No. 11 blade to split the tracheal cartilages at their midpoint. Transect the dorsal tracheal membrane with Metzenbaum scissors. Preplace, and then tie, three or four simple interrupted sutures (3-0 or 4-0 polypropylene) in the dorsal tracheal membrane. Retract the endotracheal tube into the proximal trachea during resection and placement of sutures in the dorsal tracheal membrane. Remove blood clots and secretions from the lumen and advance the tube distal to the anastomosis after dorsal tracheal membrane sutures are placed. Complete the anastomosis by apposing the split cartilage halves or adjacent intact cartilages with simple interrupted sutures beginning at the ventral midpoint of the trachea. Space additional sutures 2 to 3 mm apart. Place three or four retention sutures to help relieve tension on the anastomosis. Place and tie these sutures so that they encircle an intact cartilage cranial and caudal to the anastomosis, crossing external to the anastomotic site. Lavage the area and appose the sternohyoid muscles with a simple continuous pattern. Close subcutaneous tissues and skin routinely.
PNEUMOTHORAX
Traumatic pneumothorax is the most frequent type of pneumothorax in dogs. It most often occurs due to blunt trauma (i.e., vehicular accidents, being kicked by a horse), which causes parenchymal pulmonary damage to the lung and a closed pneumothorax. Spontaneous pneumothorax occurs in previously healthy animals without antecedent trauma and may be primary (i.e., an absence of underlying pulmonary disease) or secondary (underlying disease such as pulmonary abscesses, neoplasia, chronic granulomatous infections, pulmonary parasites such as Paragonimus, or pneumonia are present). Based on the histologic appearance of the pulmonary lesion, both cysts and bullae have been reported in dogs. Primary spontaneous pneumothorax in dogs may be due to rupture of subpleural blebs; the remaining lung tissue may appear normal. These blebs are most commonly located in the apices of the lungs. Secondary spontaneous pneumothorax is more common in dogs than the primary form.
Diagnosis
Signalment. Traumatic pneumothorax is most common in young dogs because they are more likely to be hit by cars or receive other trauma that may result in pulmonary damage. For similar reasons, males may be more commonly affected than females. Although traumatic pneumothorax occurs in cats, it is less common than in dogs. Spontaneous pneumothorax usually occurs in large and "deep-chested"; however, it may occur in small dogs. Dogs of any age may develop spontaneous pneumothorax; in one study the average age was 6.3 years (range 1 to 13 years). Male and female dogs appear to be equally affected.
History. Pneumothorax secondary to trauma usually results in acute dyspnea. The history of trauma is often vague or unknown, complicating the differentiation of traumatic from spontaneous pneumothorax. Although the history of dogs with spontaneous pneumothorax varies depending on underlying etiology, most animals present with an acute history of dyspnea. Occasionally a chronic cough or fever may be noted. Recurrence of dyspnea in an animal previously treated for pneumothorax suggests spontaneous rather than traumatic pneumothorax.
Radiography/Ultrasonography
Thoracic radiographs should be delayed until after thoracentesis in dyspneic animals. Pneumothorax usually occurs bilaterally in animals because air easily diffuses across the thin mediastinum. Pneumothorax results in an increased width of air-filled space in the pleural cavity. The most sensitive view is a horizontal-beam, laterally recumbent thoracic radiograph. On a recumbent lateral thoracic radiograph the lungs collapse and retract from the chest wall and the heart usually appears to be elevated from the sternum. This apparent elevation of the heart is not noticeable on a standing lateral radiograph. Partially collapsed or atelectic lung lobes appear radiopaque when compared to the air-filled pleural space. As the lungs collapse, the vascular pattern will not extend to the chest wall; this may be particularly noticeable in the caudal thorax on a ventrodorsal view. Radiographs should be carefully evaluated for underlying pulmonary disease (i.e., abscess, neoplasia) or associated trauma (i.e., rib fractures, pulmonary contusion). Pulmonary blebs found in some animals with spontaneous pneumothorax are seldom visible radiographically. This is probably because the large blebs have ruptured causing the pneumothorax. In such cases, surgical identification of bulla is necessary. Air-filled bullae may be incidental findings on thoracic radiographs of some animals. Pneumomediastinum is characterized by the ability to visualize thoracic structures (i.e., aorta, thoracic trachea, vena cava, esophagus) that are not usually apparent on thoracic radiographs.
Surgical Treatment
Surgical therapy of animals with traumatic pneumothorax is seldom necessary. However, non-surgical management of spontaneous pneumothorax usually results in a less than satisfactory outcome. Mechanical pleurodesis of the lungs may decrease the recurrence of pneumothorax in animals operated for spontaneous pneumothorax. Mechanical pleurodesis damages the pleura such that healing results in adherence of the visceral and parietal pleural. Postoperative pneumothorax or pleural effusion must then be prevented as they will result in separation of the parietal and visceral pleura, precluding adhesion formation.