Philip R. Fox, DVM, MSc, DACVIM, DECVIM (Cardiology), ACVECC
OVERVIEW
Coughing is associated with both respiratory and cardiovascular disease. The coughing reflex may be initiated throughout the upper and lower respiratory system (pharynx, larynx, tracheobronchial tree, and small airways). In some animals coughing is occasional and of no clinical significance, while in others, coughing is irritating and often fatiguing (both to the animal and the owner), and a harbinger of serious underlying disease. Clients may confuse coughing with gagging, wheezing, labored breathing, and reverse sneezing. Some dogs may retch or vomit after a bout of coughing and this is misinterpreted as gastrointestinal disease. Etiologies may be related to cardiovascular disorders, inflammation, neoplasia, parasitic diseases, trauma, degenerative disorders, physical causes, and allergic states. Naso-pharyngeal diseases induce gagging (simulating coughing), nasal discharge, sneezing, snorting, ptyalism, or strider; laryngeal diseases cause gagging, strider and sometimes cough. Common causes of coughing in the dog include cardiovascular conditions (left-sided heart failure; impingement on the mainstem bronchi by severe left heart enlargement; heart worm disease), large airway disease, tracheobronchitis, and pulmonary fibrosis. In cats, feline bronchial disease (including 'asthma') is relatively common.
Coughing may be associated with other clinical signs. Dyspnea or respiratory distress refers to difficult or labored breathing based upon assessment of breathing effort, respiratory rate, rhythm, and character. Affected animals typically display a standing or sitting posture (cats rest on their sternum), with neck extended and elbows adducted. Tachypnea (polypnea) relates to an increased breathing rate, which may or may not be associated with a dyspnea.
Certain generalizations have been made about coughing: tracheal disease may cause dry, honking, resonant cough (dogs) and dyspnea or strider (cats); bronchiolar disease may cause cough often followed by retching; alveolar disease may cause mild cough with dyspnea, or moist cough, gagging, and expiration of frothy fluid (pulmonary edema); cats rarely cough from pulmonary edema but do from bronchitis, asthma, heart-worm, lungworms, neoplasia, and foreign bodies. One must remember, however, that most coughs sound alike and are difficult to ascribe to a particular etiology.
THE ROLE OF THORACIC RADIOGRAPHY
Thoracic radiography provides valuable information about cardiac size, shape and contour, vascular and lung patterns, pleural changes, thoracic musculoskeletal conformation and conditions. Radiographs help confirm or exclude clinical impressions, support or reject a diagnosis, and provide medical information not otherwise suspected. They should be evaluated in context of the history, physical examination, clinical pathology and ECG. Repeat radiographic evaluations (using the same radiographic technique and positioning as the initial exposures) supply useful comparative data.
The importance of good technical quality to avoid misleading or erroneous diagnosis cannot be overstated. Two well-positioned radiographic views (a lateral projection and either dorsoventral or ventrodorsal projection) are essential for a complete evaluation. Films should be exposed at peak inspiration (poorly inflated lungs will appear increased in density [i.e., 'whiter']) using a high kVp/low mAs technique. Abnormalities of cardiac size and shape must be evaluated with the entire database. Breed conformation, state of respiration, obesity, relative state of hydration, stage of cardiac cycle, positioning errors and effusions alter radiographic appearances. Over exposure can result in loss of important information about the respiratory system; under exposure can cause the clinician to "over interpret" lung field markings. Faulty development process can adversely affect film quality.
High quality radiographs are essential for accurate diagnosis and optimal management by: 1) providing information about the topographic location, type, and extent of thoracic disease, 2) screening for many cardiopulmonary, systemic, and metabolic disorders, and 3) helping to formulate initial treatment strategies and assess response to various therapies.
INTERPRETING THE THORACIC RADIOGRAPH
Radiographic Anatomy
Radiographs identify the cardiac silhouette, great vessels, vascular patterns, large airways, lung parenchyma, pleural and extrapleural spaces. A normal cardiac silhouette does not necessarily exclude heart disease (echocardiography or angiocardiography will distinguish internal cardiac dimensions, chamber size, structure, valve morphology and cardiac function); moreover, respiratory disease cannot often be excluded on the basis of a radiograph alone.
Evaluation of the Heart and Great Vessels
In the lateral canine view, the heart is oriented at approximately a 45 degree angle, is situated between the 3rd-8th thoracic vertebrae, occupies about 3 intercostal spaces, and measures about 8.5-10.6 (average, 9.7) vertebral bodies (T4) wide using the vertebral heart score method. In the VD or DV view it has a roughly elliptical shape with a curved right ventricular and relatively straight left ventricular border. Breeds often influence anatomic contours. Anatomical structures include (clockwise); aortic arch (extending from 11 to 1 o'clock); main pulmonary artery segment (1 to 2 o'clock); left auricular appendage (2 to 3 o'clock); left ventricle (2 to 6 o'clock), and right heart (6 to 12 o'clock). In the right lateral view, the left atrium is superimposed over the caudal-dorsal one-third of the heart just distal to the tracheal bifurcation. When significantly enlarged, the left atrium may compress mainstem bronchi and contribute to coughing. In the lateral feline view, the heart is oval and narrower than the dog (2.5 to 3 intercostal spaces wide), varies from vertical to nearly horizontal, and is separated from the diaphragm by 1 or 2 intercostal spaces. In the VD or DV view, anatomic structures are situated similarly to dogs.
Abnormalities in Cardiac Size and Shape must be evaluated with the entire database. Breed conformation, state of respiration, obesity, relative state of hydration (e.g., dehydrated vs. overhydrated), stage of cardiac cycle, positioning errors and effusions alter radiographic appearances. Pleural effusions, when severe, will obscure the cardiac silhouette. In certain disorders, the heart may appear relatively normal (e.g., some hypertrophic heart diseases, small atrial or ventricular septal defects, early pericardial diseases, mild aortic or pulmonic stenosis, mild mitral or tricuspid insufficiency, myocarditis, endocarditis, early heartworm disease, cardiac neoplasia). Cardiomegaly usually results from congenital or acquired lesions causing volume overload (e.g., valvular insufficiency or shunts), pressure overload (e.g., valvular stenosis), myocardial disease (e.g., cardiomyopathy), pericardial disease, or severe respiratory conditions (e.g., cor-pulmonale). The cardiothoracic distance decreases in the DV or VD view but this can also be influenced by phase of respiration and pleural disease. Cardiac function cannot be directly assessed by radiography.
Evaluation Of Lung And Vascular Patterns
Radiographic interpretation of pulmonary disease includes a pattern-based approach to describe pulmonary changes in relation to suspected histopathologic correlates.
Alveolar patterns indicate alveolar collapse or filling (with blood, pus, or water). Characteristic findings include: 1) patchy, poorly defined, increased densities with fluffy, indistinct margins which tend to coalesce, 2) air bronchograms (i.e., air-filled [and therefore radiographically grey or black] branching tubes surrounded by abnormal radiographically opaque [i.e., whitish] lung, and 3) silhouetting of pulmonary vessels and bronchial walls by lung tissue infiltrated with fluid. Related disorders include bronchopneumonia, pulmonary edema, hemorrhage, and atelectasis.
Interstitial patterns indicate disease or perturbation of the interstitium. Characteristic findings include 1) increased nodular densities having distinct, well defined margins (e.g., neoplasia, chronic granulomas); 2) indistinct nodular margins extending into areas of focal edema or into alveoli; 3) a nonspecific localized or generalized "grayness" without distinct features, sometimes referred to as an unstructured interstitial pattern (e.g., pulmonary edema, pulmonary fibrosis, some neoplasia, interstitial pneumonia).
Bronchovascular patterns may result from increased bronchial and vascular structures or decreased vascular prominence. Hypervascularity refers to arteries and/or veins. Both may be enlarged together in states of increased pulmonary blood flow (left-to-right shunts), high output states (thyrotoxicosis, severe anemia, fluid overload), left-sided CHF from severe mitral insufficiency or canine dilated cardiomyopathy (i.e., chronic pulmonary venous dilation with secondary pulmonary hypertension). Increased pulmonary artery size and shape suggest pulmonary hypertension (usually dirofilariasis; occasionally, right-to-left shunts, idiopathic pulmonary hypertension). Pulmonary venous congestion is associated with left-sided CHF. Hypovascularity (hypoperfusion or undercirculation) creates thin arteries, veins and radiolucent interstitium and may accompany low cardiac output [shock, dehydration, caval syndrome, cardiac tamponade, acute blood loss, hypoadrenocorticism, restrictive pericarditis, severe myocardial failure), or right to left shunts. Bronchial patterns may show 1) thickened or calcified walls (appearing as parallel lines when viewed longitudinally, or as thick walled 'doughnuts' when viewed in cross section); 2) decreased, irregular luminal diameters and/or peribronchial densities. Bronchiectasis may appear as thin-walled, cylindrical or saccular bronchial dilation with enlarged bronchial lumens. Bronchoscopy or tracheobronchial lavage with cytology, culture and sensitivity, and various clinical pathology tests are often required to elucidate associated bronchial disorders. Many diseases caused mixed patterns.
LIMITATIONS OF RADIOGRAPHY
Radiography provides no direct information about internal cardiac structures; can not assess myocardial function; does not directly assess blood flow dynamics; and can infer but not verify pericardial effusion. Pleural effusions, when severe, will obscure the cardiac silhouette. Echocardiography is may satisfy these shortfalls. In certain disorders, thoracic radiographs may be unremarkable or changes in cardiac silhouette may be mild (e.g., feline myocardial diseases [particularly early]; small restrictive atrial or ventricular septal defects; early pericardial diseases with minimal effusion; mild aortic or pulmonic stenosis; trivial valvular regurgitations; myocarditis; early valvular bacterial endocarditis; early/mild heartworm disease; cardiac neoplasia with small tumors and lack of effusions. Echocardiography may be useful in certain of these disorders to evaluate cardiac chamber enlargement, ventricular wall thickness, assess valves, assess blood flow direction and quantitate gradients (with Doppler echocardiography).
| Figure 1. | 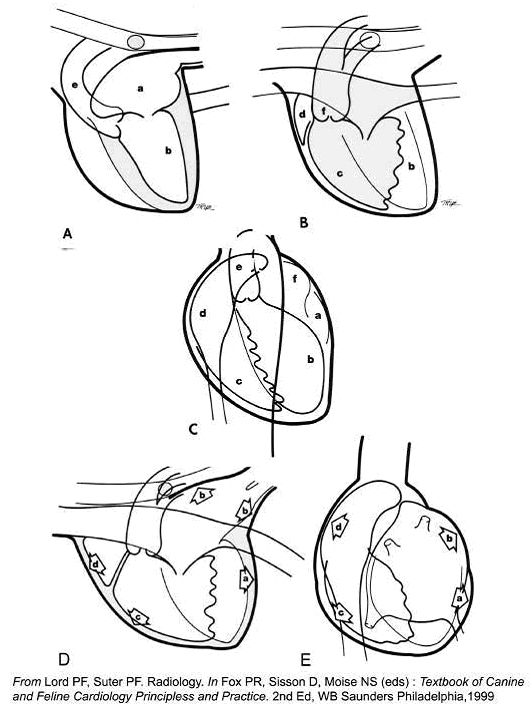
|
|
| |
A, B. Normal heart, Right lateral view. a, LA; b, LV; e, Ao; c, RV; d, RAu; f, PA
C. Normal heart, VD view. a, LAu; b, LV; c, RV; d, RA; e, Ao; f, Main PA
D. Volume overload (MR/TR), Right lateral. Right heart enlargement is present increasing sternal contact ( c ); Left hear enlargement is present causing the caudal heart border (LV, a) to enlarge, lose its convexity, and become 'straighter.' The LA enlarges (b). Tracheal elevation (b) reflects LAE and LVE
E. Volume overload. A, LV; b, LAu; c, RV; d, RA
References
1. Myer W. Diagnostic imaging in respiratory disease. In Birchard SJ, Sherding RG (eds): Saunders Manual of Small Animal Practice. 2nd Ed, WB Saunders, Philadelphia, 2000, p611
2. Lord PF, Suter PF Radiology. In Fox PR, Sisson DD, Moïse NS (eds): Textbook of Canine and Feline Cardiology. Principles and Practice. 2nd Ed. WB Saunders, Philadelphia, 1999, p 107
3. Burk R, Ackerman N. Small Animal Radiography and Ultrasonography. 2nd Ed, WB Saunders, 1996
4. Suter PF. Thoracic Radiography. A Text Atlas of thoracic Diseases of the Dog and Cat. PF Suter, Wettswil, Switzerland, 1984