D. Smeak
Veterinary Clinical Sciences, Colorado State University, Fort Collins, CO, USA
Importance of Ligations
Ligation involves the use of encircling suture material and a knot, called a ligature, to tightly occlude blood vessels in surgery. Despite the introduction of newer electrosealing devices for use in open and minimally invasive surgery now available to veterinarians for large vessel hemostasis, ligatures are still considered the gold standard method to achieve hemostasis. Ligation of solitary vessels, or multiple vessels within a pedicle (mass ligation) is used virtually every day in practice during ovariohysterectomy, castration, amputation, splenectomy, and lobectomies; therefore, creating secure ligations is one of the most critical life-saving steps in most soft tissue surgeries.
Suggested Suture Material Choice and Size for Ligation
Although a number of sutures can be used successfully to ligate a pedicle or critical blood vessel, most surgeons choose strong absorbable monofilament material (such as polydioxanone—PDS, polyglyconate—Maxon, glycomer 631—Biosyn, poliglecaprone 25—Monocryl) of 0 to 3-0 size for most small animal applications. For larger arteries, some surgeons still recommend monofilament nonabsorbable suture material, such as polypropylene. Multifilament sutures such as silk, a suture noted for its excellent handling and ligation qualities, can be used successfully for ligation but these sutures have been shown to increase the risk of suture-related wound infections. In addition, generally speaking, multifilament suture materials tend to lockup prematurely during tying (the first throw of the knot may not tighten fully around the vessel or pedicle) since the suture develops more friction between strands compared to the monofilaments. Knot ears should be cut at least 3 mm for synthetic sutures. Generally speaking, it is good practice to choose the smallest suture material size providing sufficient strength for the intended ligation.
Testing the Security of Ligations
One of the most common but dangerous ways surgeon’s attempt to “test” their ligations to be sure they are leakproof is to carefully and slowly release the clamps and any tension on the ligated pedicle and watch to see if bleeding occurs from the cut end. Realize that simply crushing the vessel or pedicle with hemostatic forceps can temporarily stop bleeding particularly when the patient is hypothermic and somewhat hypotensive. In addition, any tension on the pedicle can also temporarily occlude flow through the vessel and this can give the surgeon the false impression that “all is well” at that site. Meticulous surgeons safely practice the principles of secure ligation, rather than solely relying on whether the pedicle is found to bleed or not soon after the ligation is completed.
Rules for Consistently Secure Ligations
- Double ligate critical blood vessels or pedicles. Transfix large vessels and pedicles especially when there is no “mushroomed” wad of tissue distal to the ligation(s).
- Use a 3-forceps technique if you choose to clamp the pedicles before ligation. The transfixing ligature is always placed distal to the first ligature since this ligature requires needle penetration of the vessel, and the first circumferential ligature safely occludes the vessel first. Do not attempt to place a ligation on a vessel or pedicle close to a hemostatic clamp unless the clamp is “flashed” or loosened and the throw can be retightened. Ideally, if the clamp can be flashed, attempt to move the ligature so it falls in the crushed area of pedicle after the hemostat has been “flashed.”
- Tension on the pedicle during knot tying also tends to loosen the first throw of a ligation. This tension also tends to fan or spread out the pedicle which increases the risk of loosening of the first throw. If the first throw loosens just a small amount, this could result in fatal hemorrhage.
- Choose strong suture material with good knot security. Place firm, slow and even tension on the knot throws during tightening so the throws are squarely fashioned.
Binding or Friction Knots
Binding knots are knots on a strand that either constrict a single object or hold multiple objects snugly together. Whippings, seizings and lashings serve a similar purpose to binding knots but contain too many wraps to be properly called a knot. In binding knots, the ends of rope are either joined together or tucked under the turns of the knot. These so-called friction knots are held in place by the friction between the windings of line, or they are held in place by the two ends of the line being knotted together. Originally, these knots were designed to be performed by solo field workers to firmly close the end of burlap sacks. Binding knots were chosen because they would temporarily hold the neck of the sack tight without assistance until the knot was permanently secure with additional square throws. Some of the more common friction knots used at that time were the miller’s knot, the constrictor knot, strangle knot, the double reverse half hitch (not covered in this presentation), and the surgeon’s knot.
During surgery, once a friction knot/throw is applied and tightened firmly it should be considered only temporarily stable, additional square throws are applied on top of it to make it permanently secure. In most cases, 3–4 snug, additional square throws will secure the ligature knot. Ideal qualities of the first throw friction knot include the ability to 1) cinch down tightly and completely without prematurely locking up. This characteristic allows the surgeon to “feel” when the knot does not cinch down any further during tensioning and thereby signaling when it is tightly applied, and 2) the friction knot should resist loosening once placed allowing time for additional throws to be performed for a permanent secure knot. A surgeon’s knot is a type of friction knot created by a double twist on the first throw (called the surgeon’s throw) and it is completed with a second square, single-twist throw on top. Although the surgeon’s throw can be used successfully for ligation in practice, it is generally not recommended for this use. This risky friction knot can “lock-up” prematurely, creating a dangerous situation in which the surgeon falsely thinks the knot has been tightly applied but it is not. When the strands are tensioned on a surgeon’s throw, as the encircled tissue is tapered, the double twisted throw tends to bind up and resists further tightening. In addition, of the friction knots mentioned in this proceeding it has been shown to be the least able to resist loosening when placed under expansile force when tested in my recent knot security research project.
Recommended One- or Two-Pass Friction Knots
Friction knots commonly employed in veterinary surgery can be classified by how many passes are placed around the pedicle. One-pass friction knots are the surgeon’s knot (not recommended for ligation) and the double reverse half hitch knot. The highly dependable 2-pass friction knots commonly chosen in practice include the traditional miller’s knot and the newly introduced strangle knot.
Some surgeons choose a one-pass friction knot since it is easier to apply as it requires only one pass of the suture around the pedicle or vessel. The two pass friction knots take a bit more effort to pass twice around the pedicle but they are highly effective as first throw knots to resist loosening. Tip: For the two pass knots, complete a loose knot on the jaws of a hemostatic forceps first, and then push the loose knot down over the jaws into the appropriate position on the clamped pedicle after which fully tighten the knot. This enables construction of the knot in a site with ample room, before it is pushed down to crush the pedicle.
For the two pass knots, complete a loose knot on the jaws of a hemostatic forceps first, and then push the loose knot down over the jaws into the appropriate position on the clamped pedicle after which fully tighten the knot. This enables construction of the knot in a site with ample room, before it is pushed down to crush the pedicle.
Miller’s Knot (2-Pass Friction Knot)
A miller’s knot is the most traditionally taught friction or so-called “binding knot” used to tie-off vessels or pedicles. This knot works well on large pedicles, such as ovarian pedicles or uterine body during ovariohysterectomy, since the strands of the knot have many surfaces in contact to increase friction, and a greater surface area of compression by the multiple suture passes encircling the pedicle. This knot does not “bind up” prematurely and allows the operator to confidently know when the knot has been tensioned correctly to obstruct blood flow through the pedicle.
fig

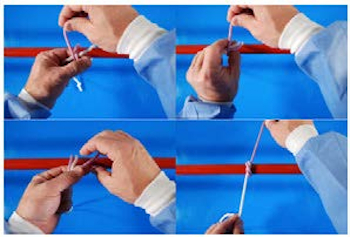
Strangle Knot Hand Tie Technique
The strangle knot is another variation of a 2-pass binding knot and can be used in lieu of a miller’s knot. The author prefers this binding knot since it tends to stay tight even when the ends are manipulated like the miller’s knot, but it is easier to tie. The only difference between this knot and the modified millers is that the strands are crossed on the first pass, and the second pass is to the left of the first formed loop.
fig