M. Kiupel1
The prognostic evaluation of canine cutaneous mast cell tumors (MCTs) is based on the assessment of complete surgical removal, their histologic appearance, including grade, proliferation index and c-Kit mutation analysis and clinical stage, especially local lymph node involvement. A fine-needle aspirate is the preferred method for the initial diagnosis of cutaneous MCTs since it provides an accurate diagnosis in approximately 95% of cases. However, accurate prognosis requires an excisional biopsy followed by microscopic evaluation. While the two-tier grading system has been applied to fine-needle aspirates and loss of granularity, presence of mitotic figures, binucleated or multinucleated cells, nuclear pleomorphism, or >50% anisokaryosis were identified as features of high-grade MCTs, approximately one third of these MCTs were falsely identified as high grade when compared to histologic grade. The initial excisional surgery also provides the best chance for a cure since the fascial planes are uninterrupted and there is no scar tissue to impede visualization of the cutaneous MCT. While different dimensions of surgical margins have been recommended for different grades of MCTs, inconsistencies in margin evaluation make it difficult to compare published methods. In general, MCTs smaller than 4 cm in diameter should be excised with at least 1 cm lateral margins and a deep margin of at least 4 mm that includes the underlying fascia or, in its absence, the superficial muscular layer. If cytology suggests a more aggressive MCT, lateral margins of 3 cm and deep margins of one fascial plane should be attempted. For those tumors that are not considered resectable, an incisional biopsy can also provide the initial diagnosis as well as allow for histologic grading. For histologic evaluation of margins, no tissue should be removed from the excisional biopsy specimen and surgical margins should ideally be inked prior to submission for histopathologic examination. We recommend margin evaluation using a combination of complete tangential margins for "cleanliness" and assessing distance of neoplastic cells to these margins based on radial sectioning of the MCT.
Evaluation of the tributary lymph node for metastasis can be challenging. Detection of sentinel nodes has been shown to more accurately determine those nodes that may potentially contain neoplastic cells. In dogs with an enlarged tributary lymph node, a fine needle aspirate of the node should be performed. However, neither cytology or histology have been able to provide consistent results regarding the local lymph node spread and different schemes have been proposed to classify those nodes that contain small numbers of mast cells that may represent early metastatic spread. We just completed a study to develop a lymph node metastatic check test based on determining quantitative expression of a number of RNAs commonly detected in neoplastic mast cells. This test will help to standardize accurate determination of metastatic spread. Regardless, lymph nodes that are confirmed or suspected to have a MCT based on cytology should be removed during the initial excisional surgery and also submitted for microscopic examination. If there is no evidence of metastasis and the cutaneous MCT is of low grade, no further staging may be needed. If the dog presents with clinical signs of vomiting or unexplained concurrent melena, an abdominal ultrasound is recommended. If lymph node metastasis is confirmed or the cutaneous tumor is graded as high grade, full staging and systemic therapy should be considered.
Regarding the selection of additional therapy beyond local excision the following points should be considered: a) Is additional local therapy indicated; b) is systemic therapy indicated; and c) is inclusion of tyrosine kinase inhibitors in systemic therapy indicated? The decision for additional local therapy is based on the evaluation of the complete surgical excision as well as histologic grading, and evaluation of proliferation indices. We recommend using the 2-tier system for MCT grading since it is currently the only system that has been shown in a number of independent studies to produce consistent results while accurately predicting biological behavior.
If histologic margins are free of overtly neoplastic cells, no further local therapy is recommended regardless of other findings. If overtly neoplastic cells extend to the examined tissue margins and the tumor is of low grade, the inclusion of additional local therapy should be considered with respect to the proliferation status of the tumor. For low grade MCTs that have a low AgNOR x Ki-67 score no local therapy is recommended since there is no difference between recurrence rates for completely excised and incompletely excised MCTs. If incomplete excision is detected for a high-grade MCT or a low-grade MCT with a high AgNOR x Ki-67 score, local therapy should be considered. Local therapy should also be considered for all high-grade MCTs with incomplete or narrow margins.
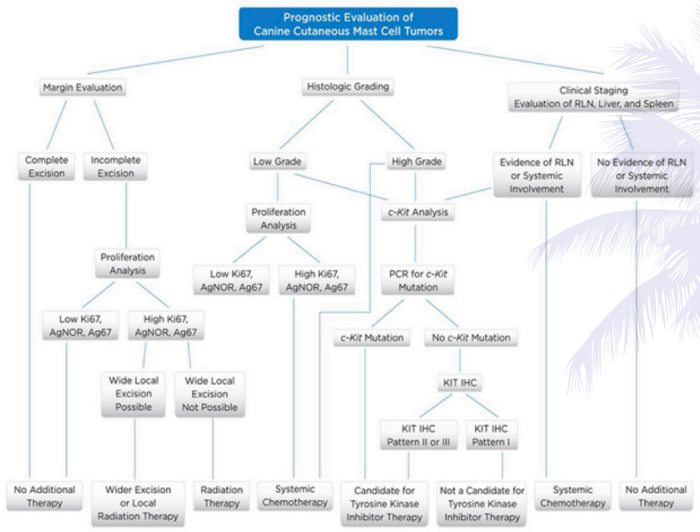
Any dog with metastasis based on staging or a diagnosis of a high-grade MCT should be considered as a candidate for systemic therapy. Regardless, as with any histologic grading system, not all aggressive MCTs can be identified by histologic grading alone and we also recommend proliferation analysis based on the combined AgNOR x Ki67 value, analysis of the KIT pattern and detection of internal tandem duplication mutations of Kit in exons 8 and 11 to identify those 5 to 15% of low-grade MCTs that may behave more aggressively. No additional therapy is indicated for histologically low-grade MCTs that have low proliferation indices including most importantly the AgNOR x Ki-67 score, that lack an activating mutation in exon 11 of c-Kit, and that have a KIT pattern 1. In contrast, systemic therapy should be considered for any dog with a low grade MCT that has either a high AgNOR x Ki-67 score, a mutation in exon 11 of c-Kit, or a KIT pattern 2 or 3.
While internal tandem duplication mutations in exon 11 have been associated with a more aggressive biological behavior, dogs with MCTs with such mutation have also been shown to respond to therapy with tyrosine kinase inhibitors. In contrast, mutations in exon 8 occur primarily in low grade MCTs with a low proliferation index and have not been associated with more aggressive behavior. Occurrence of such mutations has been suggested to indicate the potential response of such MCTs to tyrosine kinase inhibitors. Similarly, the KIT pattern of a cutaneous MCT will also help to determine its biological behavior and dogs with a KIT pattern 2 or 3 are more likely to have a mutation in c-Kit and therefore are more likely to respond to tyrosine kinase inhibitors.
While all of the methods of assessment of MCTs described above have individual merit, it is important to recognize that the prognostic value of an individual parameter is based on a statistical evaluation of a population and may not accurately predict behavior of a given tumor in a single patient. There are always exceptions in which the clinical, histologic, and molecular features of an individual MCT favor a benign course, but the clinical outcome is poor, or vice versa.
As such, patients should be evaluated on a case by case and tumor by tumor basis, and communication between clinicians and pathologists is of paramount importance. A holistic approach to prognostication and treatment selection is recommended that combines clinical assessment, histopathologic evaluation, and molecular diagnostics. Moreover, general practioners, oncologists, and pathologists should not be viewed as independent, but should work in collaboration to ensure the best possible treatment of patients.
References
1. Hume CT, Kiupel M, Rigatti L, Shofer FS, Skorupski KA, Sorenmo KU. Outcomes of dogs with grade 3 mast cell tumors: 43 cases (1997–2007). J Am Anim Hosp Assoc. 2011;47(1):37–44.
2. Kiupel M, Webster JD, Bailey KL, et al. Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet Pathol. 2011;48(1):147–155.
3. Kiupel M, Webster JD, Miller RA, Kaneene JB. Impact of tumour depth, tumour location and multiple synchronous masses on the prognosis of canine cutaneous mast cell tumours. J Vet Med A Physiol Pathol Clin Med. 2005;52(6):280–286.
4. Krick EL, Kiupel M, Durham AC, Thaiwong T, Brown DC, Sorenmo KC. Investigating associations between proliferation indices, c-kit and lymph node stage in canine mast cell tumors. J Am Anim Hosp Assoc. 2015. [Accepted for publication]
5. Smith J, Kiupel M, Farrelly J, Cohen R, Olmsted G, Kirpensteijn J, Brocks B, Post G. Recurrence rates and clinical outcome for dogs with grade II mast cell tumours with a low AgNOR count and Ki67 index treated with surgery alone. Vet Comp Oncol. 2015;3. [Epub ahead of print]
6. Webster JD, Kiupel M, Kaneene JB, Miller R, Yuzbasiyan-Gurkan V. The use of KIT and tryptase expression patterns as prognostic tools for canine cutaneous mast cell tumors. Vet Pathol. 2004;41(4):371–377.
7. Webster JD, Kiupel M, Yuzbasiyan-Gurkan V. Evaluation of the kinase domain of c-KIT in canine cutaneous mast cell tumors. BMC Cancer. 2006;1(6):85.
8. Webster JD, Yuzbasiyan-Gurkan V, Kaneene JB, Miller R, Resau JH, Kiupel M. The role of c-KIT in tumorigenesis: evaluation in canine cutaneous mast cell tumors. Neoplasia. 2006 Feb;8(2):104–111.
9. Webster JD, Yuzbasiyan-Gurkan V, Miller RA, Kaneene JB, Kiupel M. Cellular proliferation in canine cutaneous mast cell tumors: associations with c-KIT and its role in prognostication. Vet Pathol. 2007;44(3):298–308.
10. Webster JD, Yuzbasiyan-Gurkan V, Thamm DH, Hamilton E, Kiupel M. Evaluation of prognostic markers for canine mast cell tumors treated with vinblastine and prednisone. BMC Vet Res. 2008;13(4):32.