The Practice Success Prescription: Team-Based Veterinary Healthcare Delivery by Drs. Leak. Morris Humphries
Thomas E. Catanzaro, DVM, MHA, FACHE, DACHE
If practice leadership and business management were easy, there would not be the racks and shelves of texts on the subject in every bookstore. There is no one best answer! - Dr. Tom Cat
The reason people have written books are as many as the authors. Each person has a personal belief why his or her thesis may be useful to others. In my case, it is the ongoing repetition by my colleagues, observing a series of paradigms and habits that limit their ability to make their practices prosper as they wish they would.
This current thesis came to the forefront during a multi-city speaking tour in Australia, and then was "rammed home" by two following events: a VCI Shirt Sleeve Seminar® in Denver, and an AAHA Veterinary Management Session I facilitated.
At the VCI Shirt Sleeve Seminar® in Denver, our new employee Erin was attending for the first time. She made the following comment to a group of our consultants, "There is a lot more young staff here than had I expected"
The response was quick from one of our consultants, "That is because most practices do not earn enough income to pay their employees enough to allow them to grow old in their jobs."
At the Veterinary Management Session I facilitated at AAHA, a group of fifty-one people from across the USA attended to learn to be better managers, of which about twenty percent were veterinarians. I was explaining the principle and programs of team-based healthcare delivery multi-tasking training techniques (mt3), which allows a practice to be productive, without requiring the veterinarian to be omnipresent. Some attendees refused to listen to the principles, and wanted to debate state, practice, and personal differences, and when asked, knew the systems being discussed would never work in their practice, for multiple reasons:
 The example used did not fit their situation like a calf-skin glove.
The example used did not fit their situation like a calf-skin glove.
They would never have enough staff.
Their facility was too small, too old, or too whatever to allow it to work.
The staff could not be trusted to work independently.
Clients would never stand for it.
Doctors would not let go of the process.
The obvious answer to these excuses: Whether you think you can, or whether you think you can't, you will make it come true!
The sequential encounters got me to thinking about our profession, and how we got to where we are. I had an epiphany.
Many of us had veterinary medicine as a dream to some it was a passion, and a few like myself, a later-in-life discovery. Then getting into veterinary medicine became a mission, to some it became a quest, and to a few, a negotiation. Once we entered the learning phase, for many it became a challenge, yet to some it was an ordeal, and for most, a rewarding adventure of skills and knowledge acquisition in the healing arts.
Then we entered a practice. I guess we call it "practice" because most believe we will never get it all "right". Nevertheless, some entered a profession, some entered a calling, and some entered a workplace. The dichotomy was becoming evident. Seldom did anyone enter a business.
Watson and Crick had it right. All life depends on a double-helix. In this case, one strand is our professional mission, and the other is our business mission. Veterinary teaching hospitals ignore the business strand of this double-helix of veterinary practice life. Therefore, the "students" do not really understand the business of veterinary medicine on graduation. Most of the academic professors are "tenured", so they do not even worry about staying employed, much less being profitable for the hospital in which they work.
This chapter is specifically designed to address the business of veterinary medicine: the ability to effectively serve a community, earn a living commensurate with the educational and investment commitment of the ownership, and employ people at a reasonable level of compensation so they can make their job a career.
The Business Operations
The business of a veterinary practice starts when the "would be" practice owner establishes a business plan and takes it to the bank for a loan. Thirty years ago, bankers wanted to lend money to veterinarians to get them to come to their town, and the red carpet was rolled out in most communities. Now, in most cases, you must prove to the bank that you do not need the money before they will lend it to you.
If you have ever developed a business plan, you probably understand the role of other "business" professionals, what we call the Business Advisory Team:
A veterinary-savvy attorney
A trusted financial planner (CFP).
A tax accountant with healthcare clients.
A personal banker.
And if one is lucky, a diversified veterinary-specific consulting team.
The amazing thing is that while a business plan usually includes a three-year program-based budget, which is what income you are expecting to earn compared to the expected expenses, as soon as the loan is obtained, the budget most often goes into oblivion, never to be used as a business tool again.
In the beginning, the practice is totally focused on the community and front-door swing rate. What a great concept! There is no "doctor-to-staff" ratio, there is "What can we afford with this caseload?" form of operational logic. Again, what a great concept! Let's look at a typical practice, using a bubble diagram:
Click on the figure to see a larger view
| Figure 22: Zoning a Practice | 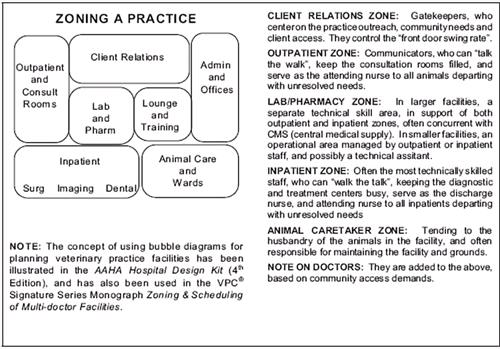
|
|
| |
While the above facility zoning stresses the role of the staff members to operate and maintain the facility, in the grand scheme of things, we all know that the doctor comes first in establishing a veterinary practice. Or more accurately in this new millennium, they used to come first. Now the business comes first, since a portion of the new practices are not even owned by veterinarians, and the bank wants the business plan, not the diploma, before lending money. This is one reason we have clearly stated that the doctor-centered veterinary practice is dead, although some have not yet accepted this fact. Look at the above diagram, and assume the following staffing:
One client relations specialist.
One outpatient nurse technician (OPNT) with three consult rooms.
One OPNT assistant in the pharmacy area to count pills and help restrain outpatient animals.
One inpatient nurse technician (IPNT) with surgery, dentistry and imaging areas.
One IPNT assistant, who also acts as an animal caretaker.
Again, no doctors are yet added. But let's assume there is an owner who has established inviolate core values, progressive and consistent standards of care, a clear mission focus, and has trained and empowered the above staff to operate the facility to achieve the business outcomes. We can the add relief (locum) doctors:
One doctor: Outpatient 8:00-10:30 a.m.; inpatient 10:45 a.m. - 2:45 p.m., including a bite of lunch; then back to outpatient 3:00 p.m.-close. Staff ratio is five to one.
Two doctors: One on outpatient duty 8:00 a.m. - 1:00 p.m., concurrent with inpatient 8:00-noon, including a bite of lunch. Then the morning inpatient becomes afternoon outpatient until close, and the morning outpatient has a bite of lunch, then becomes inpatient until all caseload has been completed. Staff does not change, so ratio is now two-point-five to one.
Add a half-time surgeon doctor: Keep the a.m.- p.m. two-doctor rotation, so we need to add a half-time surgery nurse. Staff ratio is six to two-point-five.
Instead of a half-time surgeon, add an evening/third doctor: On Tuesdays and Thursdays work 11:00 a.m. - 8:00 p.m., with surgery noon 3:00 p.m., 3:00-4:00 p.m. food and phone, and 4:00-close outpatient. On Fridays work 8:00 a.m. - 6:00 p.m., as the one doctor schedule. Saturdays, 8:00 a.m. - 3:00 p.m. with no inpatient time, and we would need to add a full-time nurse instead of a part-time surgery nurse. Staff ratio is now two to one.
What we have illustrated above is that, as a business, a facility is doctor-staffed, based on client access demand, and the facility operations can be handled by a core team of outcome-accountable veterinary staff. Again, the training and development details have been provided in the VCI® Signature Series Monographs Orientation and Training and Zoning & Scheduling of Multi-doctor Facilities.
Hold it folks, I almost got carried away. If we are talking about business operations, we now have the cart before the horses. The vision of the practice must come first, the picture painted so vividly, exciting the hearts and minds of all who hear it, and defined so clearly by the leadership that everyone wants to gain that horizon. In the VCI® Signature Series Monograph Leadership Action Planner to develop the core values and vision, the core values are inviolate, and cause the development of a "safe haven" for staff to make unilateral decisions for the good of the practice, clients, patients and operations. To develop the behavior and skills needed to lead others, the VCI® Signature Series Monograph Leadership Principals and Skills provides some of the basics for the practice leadership and doctors. The VCI® Signature Series Monograph Professionalism, Bio-ethics, and Problem-solving is helpful to develop a balanced practice philosophy. It also maybe needed by the coordinators and doctors to ensure a level playing field in the team-based healthcare facility operations. Concurrently, the VCI® Signature Series Monographs Building a Bond-centered Practice, for client-centered patient advocacy development at all levels, and Standards of Patient Care, to achieve a consistency needed for acceptance by clients and staff alike, help provide the basics for the team-based healthcare delivery operations for most practices. Diagrammatically, the flow of operational attributes can be illustrated, as shown in the Leadership Impact on Practice Flow chart.
Now that the concept of operations has been secured, we must put in place the business aspects that support and track the healthcare delivery commitment and team activities.