Urethral Obstruction: Techniques to Relieve Obstruction and Management of the Patient
University of Georgia, College of Veterinary Medicine, Department of Physiology and Pharmacology
Athens, GA, USA
OVERVIEW OF URETHRAL OBSTRUCTION
Urethral obstruction is a life-threatening situation. Complete urethral obstruction in a patient for only 2 or 3 days can be fatal due to renal dysfunction and retention of metabolic wastes, especially potassium and metabolic acids. Therefore, reestablishing urine outflow should be considered an emergency, and appropriate steps should be taken to the correct the situation.
There are many potential causes of urethral obstruction, however, this discussion will focus on nonsurgical management of urethral obstruction due to uroliths (dogs and cats) and intraluminal plugs (cats).
MANAGEMENT OF CANINE URETHRAL OBSTRUCTION
"There are some patients whom we cannot help, but there are none that we cannot harm." A.L. Bloomfield
The goal of every veterinarian is to help their patients, however, we should not loose site of the fact that in our desire to help our patients, we have the potential to cause significant harm. It is obvious that relieving complete urethral obstruction is essential for saving a patient's life, but it is important that we don't create a cascade of other problems in the process that could be avoided with careful planning.
SUMMARY OF MAJOR STEPS FOR RETROGRADE UROHYDROPROPULSION IN DOGS
1. Verify and localize the urethroliths.
2. Decompress the urinary bladder by cystocentesis. Save aliquots of pre-treatment urine for urinalysis and urine culture.
3. Avoid forceful catheterization.
4. Lubricate the urethral lumen to facilitate retropropulsion of urethroliths.
5. Perform retrograde urohydropropulsion.
6. Minimize pain and trauma to various components of the urinary tract as well as iatrogenic urinary tract infections.
7. Repeat lateral abdominal radiograph to ensure urethral stone(s) have been successfully retropulsed back into the bladder.
Obtain Appropriate Diagnostic Information
When patients present with urethral obstruction, there is tendency to want to immediately attempt urethral catheterization and try to relieve the obstruction, and then perform diagnostic tests, rather than the other way around. This approach may work in some situations, however, if a case is particularly challenging or there are complications, you have lost your window of opportunity to obtain pretreatment diagnostic information that may have provided valuable insight about the patient's problem, as well as how best to manage it. Rarely is a patient's condition so critical that you cannot safely perform a few diagnostic tests before attempting to relieve the obstruction.
Step 1. Verify and Localize Urethroliths
1. Palpation of urethra, including rectal palpation
This can provide you with valuable information that may not be detected with survey radiography, such as palpating a mass in the urethra. It is unfortunate if a dog is taken to surgery to remove bladder stones, only to find out that the main problem was transitional cell carcinoma of the urethra.
2. Radiography
Appropriate survey or contrast radiography or ultrasonography should always be performed to localize the site(s) of obstruction, as well as the number, size, and surface characteristics of urethroliths.
The majority of times, a lateral survey abdominal radiograph will provide you with this information. It is very important that you include the entire urinary tract, including all of the lower urinary tract, on the radiograph. It is also helpful if you put one hind leg slightly in front of the other so that you are not trying to visualize an area of the urethra that is in the field of both hindlegs.
Although survey abdominal radiographs will not detect all uroliths, the majority of the common uroliths (struvite, calcium oxalate, cystine) are radiodense to some degree, with the exception of some urate uroliths that are radiolucent.
|
Mineral Type |
Radiographic Density* |
|
struvite |
+ to ++++ |
|
calcium oxalate dihydrate |
++++ |
|
calcium oxalate monohydrate |
+++ |
|
cystine |
+ to ++ |
|
urate |
0 to ++ |
*0 = radiolucent; ++++ = radiographic density of bone
Step 2. Decompress the Urinary Bladder by Cystocentesis. Save Aliquots of Pre-Treatment Urine for Urinalysis and Urine Culture
If the patient's urinary bladder is enlarged, a decompressive cystocentesis should be performed prior to attempting to relieve the obstruction to prevent iatrogenic overdistension of the bladder. Although there are potential risks of performing decompressive cystocentesis, such as extravasation of urine into the bladder wall or peritoneal cavity or injury to the bladder, if appropriate techniques are used, these complications have been an uncommon exception rather than the rule. Far greater number of complications occur when relief of urethral obstruction is attempted in a patient with an already overdistended urinary bladder. You are more likely to rupture the urinary bladder if you force fluid into an already overdistended urinary bladder than if you carefully remove most of the urine prior to relieving the urethral obstruction.
Advantages of performing decompressive cystocentesis prior to relieving the urethral obstruction include:
1. Obtaining a pre-treatment urine sample suitable for urinalysis and urine culture. Solutions used to flush the urethral lumen alter the composition of urine in the bladder and result in alterations in results of diagnostic tests.
2. By removing most, but not all of the urine from an overdistended urinary bladder using decompressive cystocentesis provides a mechanism to temporarily ameliorate the discomfort to the patient, as well as prevent the continued adverse effects of obstructive urethropathy.
3. Decompressive cystocentesis decreases the amount of resistance to retrograde movement of urethroliths into the bladder lumen.
Technique of Decompressive Cystocentesis
Supplies 22-gauge needle
 flexible IV extension set
flexible IV extension set
3-way stopcock
6 cc syringe
large (>20 cc) syringe
alcohol
Attach the 22-gauge needle to the flexible IV extension set. Attach a 3-way stopcock to the other end of the extension set, and attach your syringes to the 3-way stopcock. Disinfect the skin over the area where you will be performing the decompressive cystocentesis. Attaching the needle to an extension set rather than directly to a syringe allows you to remove large volumes of urine from the bladder without having to repeatedly stick the bladder with a needle. The extension set also enables the person performing the cystocentesis to keep the needle still while the person collecting urine in syringes can move the syringes as needed. The 3-way stopcock allows you to interchange between the syringe used to obtain a diagnostic urine sample, and the larger syringe used to empty the urinary bladder. It also allows you to empty the large syringe multiple times during the procedure without allowing urine to drip out of the IV extension set.
| 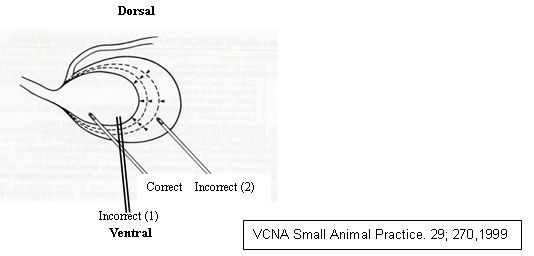
Proper insertion of the needle into the urinary bladder will facilitate removal of urine while minimizing trauma to the bladder. |
|
| |
Correct and incorrect sites of insertion of a needle into the bladder for the purpose of performing a decompressive cystocentesis in an overdistended bladder. The needle should not be inserted perpendicular to the bladder [incorrect (1)] because as the bladder is emptied, the needle resists contraction of the bladder and can result in trauma to the bladder wall. Inserting the needle too caudally in the bladder [incorrect (2)] will require reinsertion of the needle as the bladder in emptied.
As you are emptying the bladder, keep track of how much urine (mls) you have removed. As you are unobstructing the patient by flushing fluid into the bladder, always keep track of how much fluid you have flushed back into the bladder. After you have performed a decompressive cystocentesis, you have a weakened area in the bladder wall. As a result, you do not want the urinary bladder to become overdistended again, and therefore, always flush a smaller volume of fluid back into the bladder than the volume of urine you removed during decompressive cystocentesis. If you have not successfully relieved the urethral obstruction but have reached the limit of fluid you can flush into the bladder, perform another decompressive cystocentesis before attempting to relieve the obstruction further.
Step 3. Avoid Forceful Catheterization
Never try to relieve urethral obstruction by using the catheter to "push" the stone back into the bladder. This can result in severe trauma and tears to the urethra.
Step 4. Lubricate the Urethral Lumen to Facilitate Retropulsion of Urethroliths
Lubrication of the urethra and urethroliths should be done prior to attempting retrograde urohydropropulsion. Often times the urethral mucosa is swollen and inflamed and lubrication may facilitate movement of the urethral stones. Occasionally failure to lubricate the urethra may result in the inability to successfully flush the stones back into the bladder.
Cleanse the tip of the penis with warm water prior to catheterization. A liberal quantity of a 1:1 ratio mixture of sterile 0.9% NaCl (of LRS) and sterile aqueous lubricant are used as the initial solution you flush into the urethra.
Technique for mixing sterile 0.9% NaCl (or LRS) with sterile aqueous lubricant.
(A) Partially fill one syringe with sterile 0.9% NaCl and the other syringe with sterile aqueous lubricant. Connect the two syringes using a 3-way stopcock. (B) Inject the contents of the syringes back and forth between the two syringes (C) until the solution is well mixed (D). Using a 3-way stopcock allows mixing of the materials without loss of sterility. Insert a red rubber catheter to the site of obstruction, and while occluding the tip of the penis, generously lube the urethral lumen with the mixture. Occasionally this procedure alone may result in the stones being flushed back into the bladder.
Step 5. Perform Retrograde Urohydropropulsion
Depending on the severity of the obstruction, patient demeanor, and level of patient discomfort, sedation or general anesthesia may be warranted. If an uncooperative dog is an anesthetic risk because of a uremic crisis or other concurrent diseases, topical application of lidocaine gel to the urethral mucosa may provide some relaxation of the urethra, however, generally more relaxation will be provided using sedation or general anesthesia.
Procedure in Male Dogs
1. Lubricate urethra by injecting a liberal quantity of the 1:1 ratio mixture of sterile 0.9% NaCl and sterile lube (A).
2. Next, an assistant should insert a gloved index finger into the rectum and firmly occlude the lumen of the pelvic urethra by applying digital pressure against the ischium through the ventral wall of the rectum (B).(this position is referred to as the "butt person"). Occasionally, the urethra slips out from under the finger. In these situations, if the dog is large enough, two fingers can be inserted rectally, and one finger is used to stabilize the position of the urethra while the other finger is used to occlude the pelvic urethra. Complete occlusion of the pelvic urethra is essential for successful retropulsion of urethral stones back into the urinary bladder.
3. A flexible red rubber catheter attached to a 35 to 60 ml syringe filled with sterile 0.9% NaCl or LRS is inserted to the point of obstruction in the urethra (do not use polypropylene catheters because they are more irritating to the urethral mucosa and more likely to induced trauma because of their rigidity).
4. The tip of the penis should be occluded around the catheter by using some gauze pads to apply pressure to the tip of the penis (D). As a result of step 3 and step 4, a portion of the urethra from the external urethral orifice to the boney pelvis becomes a "closed system".
5. With the closed system in place, saline should be injected into the urethra until marked distension of the urethra is detected. Generally enough pressure will not be achieved in the urethra unless the barrel of the syringe is placed on the table and applying pressure to the syringe by putting your weight on the syringe. Failure to create sufficient pressure in the urethral lumen is one of the most common causes of failure to flush the urethroliths back into the urinary bladder. The chance of rupture of the urethral lumen by intraluminal pressure generated by this technique is minimal. Generally fluid will either leak out at the tip of the penis or go past the point where the pelvic urethral is being occluded. Although theoretically someone could create enough pressure to cause the urethra to tear, I have never observed or heard of this happening.
6. When adequate urethral pressure is achieved, the person holding the syringe and applying the fluid through the catheter tells the "butt person" to let up on the pelvic urethra. The catheter person continues to flush fluid through the urethra while this is occurring (D). When properly coordinated, this step forcibly advances fluid and hopefully the urethrolith(s) toward or into the urinary bladder. It is very important to keep track of how much fluid is being flushed into the bladder so that overdistention of the urinary bladder does not occur.
7. If successful retropulsion of urethral stones does not occur after the first attempt, the procedure can be repeated as needed.
Step 6. Minimize Pain and Trauma to Various Components of the Urinary Tract As Well As Iatrogenic Urinary Tract Infection
Because catheterization is not a sterile procedure and generally patients have inflamed and irritated tissues, it is recommended that patients be started on prophylactic antibiotics even if no bacteria are found when the urine is cultured.
Step 7. Repeat Abdominal Radiographs to Ensure Successful Retropulsion of Urethral Stones Back Into the Bladder
Procedure in Female Dogs
The procedure in female dogs is very similar to that in male dogs with a few exceptions.
1. After urethral lubrication, the catheter is inserted to the site of obstruction.
2. Digital urethral pressure is applied rectally over the catheter just distal to the site of obstruction.
3. Generally it is easier to flush urethral stones back into the bladder in a female dog than in a male. But just as in the male, it is important to keep track of how much fluid you have flushed into the bladder, and repeat a decompressive cystocentesis if necessary to prevent overdistention of the urinary bladder.
4. Steps 6 and step 7 listed for the male dog are also done for the female dog.
Feline Urethral Obstruction
Summary of Major Steps for Management of Feline Urethral Obstruction
1. Verify and localize whether urethral obstruction is due to uroliths or a urethral plug by taking a survey abdominal radiograph.
2. Sedation is generally necessary for male cats.
3. Decompress the urinary bladder by cystocentesis. Save aliquots of pre-treatment urine for urinalysis and urine culture.
4. Avoid forceful catheterization. Cleanse tip of penis prior to catheterization, and apply sterile lube to the urinary catheter before inserting in urethra.
5. If the cause of urethral obstruction is due to urethroliths:
a. Lubricate the urethral lumen to facilitate retropropulsion if obstruction (this step is similar to that used for dogs with urethral obstructions due to urethroliths).
b. Next, perform retrograde urohydropropulsion. Unlike in the dog, generally only the tip of the penis will be occluded when performing this procedure in a male cat.
6. If obstruction due to urethral plug, do not lube the urethral lumen.
a. Apply gentle external palpation to the distal urethra and then gently compress the urinary bladder. Occasionally this will be all that is needed to relieve the obstruction.
b. If urethral obstruction persists, perform antegrade urohydropropulsion
7. Minimize pain and trauma to various components of the urinary tract as well as iatrogenic urinary tract infection.
Urinary Catheter Selection
The anatomy of the urethra in the male cat necessitates that proper technique is used during catheterization and care is taken to avoid iatrogenic trauma to the urethra and the tip of the penis. Meticulous aseptic and gentle "feather touch" techniques should be used. Therefore, urinary catheter selection is one very important way to reduce the risk of complications associated with catheterization.
Disposable polypropylene "tom cat" catheters are commonly used when catheterizing male cats. Unfortunately, these catheters can induce trauma along any point in the urethra, and the material they are made from causes more inflammation and swelling than do red rubber catheters. However, one of the best catheters to use for unobstructing male cats are the "Minnesota Olive-Tip Urethral Catheters." These catheters were developed by Dr. Carl Osborne at the University of Minnesota.
The "Minnesota Olive-Tip Urethral Catheters" are 22-gauge catheters that are available in three different sizes (0.5, 1.0, and 1.5 inches). They can be purchased from Enjay International, Inc, Box 1835, Glendora, California 91740. They can also be purchased from JA Webster, Inc (1-800-225-7911), where they are called "Osborne Feline Urethral Catheters." Prices in 1999 for each catheter was $7.88, however, the catheters can be resterilized and reused multiple times.
The catheters come in three different lengths and have an open ended olive tip, which makes them ideal for flushing uroliths into the bladder or flushing urethral plugs out of the urethra. The material they are made out of is less irritating to the urethra than polypropylene. Because of the rounded "olive tip", they are also less likely to induce urethral trauma than are "tom cat" catheters. When unobstructing a cat, the olive tip catheter is connected to an IV extension set that is connected to a syringe containing either sterile 0.9% NaCl or LRS. The sterile fluid acts in much the same way as a water pick does.
Although these catheters are not long enough to reach the bladder, and therefore cannot be used as an indwelling urinary catheters, they are ideal for relieving urethral obstruction with the least amount of trauma.
Post-Obstruction Management
Although polypropylene catheters induce more inflammation than red rubber catheters or olive tip catheters, the red rubber catheters and olive tip catheters are still foreign materials when inserted into the urethra, and therefore induce inflammation and swelling. After a urinary catheter has been left in place for a day or more, it is not uncommon to have urethral spasming occurring after the catheter is removed. It is often difficult to tell whether the cat has reobstructed or is just having urethral spasming when it is having difficulty urinating once the catheter has been removed. For these reasons, I do not automatically leave an indwelling urinary catheter in all cats that I unobstruct. For example, if a cat was obstructed with urethral stones and I have successfully retropulsed the stones back into the bladder, in general, I do not leave an indwelling urinary catheter in these cats unless the cat repeatedly reobstructs with the stones.
Other Situations in Which an Indwelling Urinary Catheter is Warranted Include:
1. If the cat is likely to undergo post-obstructed diuresis, I will leave an indwelling urinary catheter in these cats for a couple of reasons.
a. These cats can produce very large quantities of urine, and monitoring urine output assists with providing adequate amounts of fluids to keep up with these losses.
b. Because of the very large volume of urine being produced, if these cats reobstruct and it is not detected immediately, the volume of urine they are producing may cause rupture of the urinary bladder.
2. If the cat has a lot of crystalline material in it bladder, sometimes I may leave an indwelling urinary catheter in for a day or so. However, I don't always leave an indwelling urinary catheter in these cats. I may flush the urinary bladder well, and attempt to dilute out the remaining crystalline material by administering either IV or SQ fluids. If the cat does reobstruct, then an indwelling urinary catheter may be necessary.
Other Important Points to Regarding Indwelling Urinary Catheters
1. If you must place an indwelling urinary catheter, use either a 3.5 fr or 5.0 fr red rubber catheter and not a polypropylene tom cat catheter.
2. Maintain a closed system with all indwelling urinary catheters.
3. Do not over insert the urinary catheter. The tip of the catheter should be just inside the bladder but not inserted so far in the bladder that is causes irritation to the bladder wall by rubbing on the wall. One of the easiest ways to achieve proper placement of the catheter without over inserting it is to gently aspirate back on the syringe as you are backing the catheter out of the bladder. If you are in the bladder, you should get urine or LRS, etc when you aspirate back. However, eventually the catheter will enter the proximal urethra, at which point you will get negative pressure when you aspirate back on the syringe. At this point, advance the catheter a very small amount back into the bladder, which will result in the catheter tip just slightly inside the bladder but not over inserted.
4. Always culture the urine right before you remove the urinary catheter.
Other Important Points to Remember when Managing Either a Dog or Cat with Urethral Obstruction
1. If you remove any uroliths, always submit them for analysis no matter how many times the animal has had previous episodes of urolithiasis. Urolith composition can change between episodes.
2. If you flush out a urethral plug, place it in a sterile red top vial and submit to the Minnesota Urolith Center for analysis. Although the vast majority of urethral plugs in cats composed of crystals will contain struvite crystals, urethral plugs composed of calcium oxalate crystals have been documented.
3. Appropriate long-term management is dependent upon arriving at a correct diagnosis.