June, 2001
Signalment, History, Physical Examination Neurological Examination Tests Performed Case Summary and Diagnosis
Signalment, History, Physical Examination
 Signalment: This patient is a ten-month-old, spayed female Rottweiler
Signalment: This patient is a ten-month-old, spayed female Rottweiler
History: Progressive ataxia, thoracic limb weakness and apparent cervical pain for past three months. The owners noted that the gait "has always been different".
Past Medical History: No history of trauma or illness was reported by the owners.
Medications: No medications have been given
Physical Examination
General: Body weight 22 kg, rectal temperature 38.3; heart rate 120/m; rhythm regular, femoral pulses equal and synchronous. Respiratory rate: panting; Mucous membranes pink, capillary refill time < 2 sec.
Alert and responsive, body condition score 5 / 9
Integument: No abnormalities noted.
Eyes, ears, nose and throat: No abnormalities noted.
Cardiopulmonary, abdominal cavity, musculoskeletal, lymph nodes: No abnormalities noted.
[Top]
Neurological Examination
Consciousness: Alert, responsive.
Posture: N; Falling, rolling: Absent; Righting reactions: N; Tremor: None
Circling: Not observed
Gait:
Postural and Placing Reactions:
Proprioceptive placing: Slow in all four limbs
Visual and tactile placing: Not examined
Hopping, hemistand/walk: Slow in all four limbs.
Wheelbarrowing: Unable to evaluate properly, fore limbs or hind limbs
Spinal (segmental) reflexes: (N=normal; D= depressed; A= Absent; I= increased;)
Forelimbs:
 Tendon Reflexes: Extensor Carpi: N: Biceps brachii: N; Triceps brachii: N
Tendon Reflexes: Extensor Carpi: N: Biceps brachii: N; Triceps brachii: N
Flexion Reflexes: N
Crossed Extensor Reflexes: Absent clinically
Pelvic limbs:
Tendon Reflexes: Quadriceps: N; Gastroc/Dig. flexors: N.
Crossed Extensor Reflexes: Absent clinically
Perineal Reflexes: N
Cutaneous Trunci Reflexes: Present in all normal segmental levels.
Painful Stimulation: Normal withdrawal responses.
Cranial Nerves
I: Not tested
II: Vision apparently normal.
III, IV, VI: Pupils equal, normal direct and indirect pupillary light reflexes. Normal ocular positions and movements.
V: Normal
VII: Normal
VIII: No head tilt; Physiological Nystagmus present. No spontaneous nystagmus; no strabismus, Audition apparently normal.
IX, X, XI: Normal swallowing action in response to stimulation.
XII: Tongue: Normal position, symmetry, movements.
[Top]
Tests Performed
Hematology, Chemistry and Urinalysis
Clinical Chemistry Laboratory Results
|
Constituent |
Patient's Results |
Units |
Reference Range (Dog) |
|
Alk. Phosphatase |
60 |
U/L |
15-127 U/L |
|
ALT (SGPT) |
42 |
U/L |
19-70 |
|
Ammonia |
|
mg/dl |
0-92 |
|
AST (SGOT) |
38 |
U/L |
15-43 |
|
Bile acids: |
|
fasting |
|
micromol/L |
0-12 |
|
post-prandial |
|
micromol/L |
0-16 |
|
Bilirubin: direct |
|
mg/dl |
0-0.1 |
|
Bilirubin: total |
0.2 |
mg/dl |
0-0.4 |
|
Blood urea nitrogen (BUN) |
18 |
mg/dl |
8-31 |
|
BUN/creatinine ratio |
20 |
|
6-25 |
|
Calcium |
10.2 |
mg/dl |
9.9-11.4 |
|
Cholesterol |
249 |
mg/dl |
135-345 |
|
Creatine kinase |
|
U/L |
46-320 |
|
Clotting: |
|
PT |
|
SEC |
7.5-19.5 |
|
PTT |
|
SEC |
9-12 |
|
PIVKA |
|
SEC |
15-18 |
|
FDP |
|
|
<10 |
|
Creatinine |
0.9 |
mg/dl |
0.8-1.6 |
|
Glucose |
105 |
mg/dl |
70-118 |
|
Electrolytes: |
|
Anion gap |
10 |
mmol/l |
12-25 |
|
Chloride |
115 |
mmol/l |
105-116 |
|
CO2, total |
21 |
mmol/l |
16-26 |
|
Potassium |
4.0 |
mmol/l |
4.1-5.3 |
|
Sodium |
144 |
mmol/l |
145-154 |
|
Lipase |
|
U/L |
0-500 |
|
Magnesium |
|
mg/dl |
1.2-2.4 |
|
Phosphorus, inorganic |
4.0 |
mg/dl |
3.0-6.2 |
|
Proteins: |
|
Albumin |
3.5 |
g/dl |
2.9-4.2 |
|
A/G ratio |
1.6 |
|
0.6-1.2 |
|
Globulin |
2.2 |
g/dl |
2.3-4.4 |
|
Total protein |
6.5 |
g/dl |
5.4-7.4 |
|
Thyroid: |
|
Thyroxine T4 |
|
micrograms/dl |
1.0-3.6 |
|
Free T4-EQ.D. |
|
ng/ml |
1.0-3.5 |
|
TSH-Canine |
|
mU/L |
2-30 |
|
Tri-iodothyro. T3 |
|
ng/dl |
75-150 |
|
Triglycerides |
|
mg/dl |
19-133 |
Hemogram Results
|
Parameter |
Patient's results |
Reference Values (Dog) |
|
Erythrocytes |
6.93 |
5.5-8.5 million |
|
Hemoglobin (Hb) |
17.2 |
12.0-18.0 g/dl |
|
Hematocrit |
45 |
37-55% |
|
Mean corpuscular volume |
69.3 |
62-77 fl |
|
Mean corpusc. Hb |
24.8 |
33-37 g/d |
|
Mean corpusc. Hb conc. |
35.8 |
21.5-26.5 pg |
|
Reticulocytes |
- |
0.5-1 % |
|
Leucocytes |
10800 |
6000-17000/microliter |
|
Band |
|
0-300/microliter |
|
Neutrophils |
6804 |
3000-11500/microliter |
|
Lymphocytes |
2700 |
1000-4800/microliter |
|
Monocytes |
756 |
150-1350/microliter |
|
Eosinophils |
540 |
100-1250/microliter |
|
Basophils |
0 |
Rare |
|
Platelets |
356,000 |
200-500x1000 |
|
Icteric Index |
|
2.0-5.0 |
|
Plasma proteins |
7.4 |
6.0-8.0 |
|
Fibrinogen |
300 |
200-400 mg/dl |
|
Protein:fibrinogen |
|
>15:1 |
Cerebrospinal Fluid Studies
Cerebrospinal Fluid: Total and Differential Cell Counts; Total Protein
Fluid from: Lumbar region
Gross appearance: Colorless
Specific Gravity: 1.005
Protein: 43 mg/dl
Total erythrocytes: 1953/uL
Total nucleated cells: < 5/uL
Differential Nucleated Cell Counts:
Neutrophils: 6%
Monocytes: 47%
Mature lymphocytes: 6%
Imaging
Plain Radiograph (1 film) and Myelography (6 films)
Click on an image to see a larger view.
| Figure 1. | 
|
|
| |
| Figure 2. | 
|
|
| |
| | Figure 3. | 
|
|
| |
|
| Figure 4. | 
|
|
| |
| | Figure 5. | 
|
|
| |
|
| Figure 6. | 
|
|
| |
| Figure 7. | 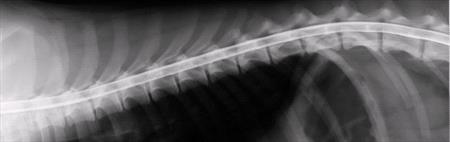
|
|
| |
| Figure 8. | 
|
|
| |
Survey Radiographs: Please note: Only one suspicious area was found on the pre-myelographic survey films. That film is not shown here but is included with the myelographic films above.
[Top]
Case Summary and Diagnosis
The clinical signs in this case indicated a cervical myelopathy. Diagnostic imaging revealed compression of the dorsal and lateral aspects of the spinal cord at vertebral level C 2-3. At laminectomy, a fibrous mass was removed. Histopathology revealed the mass to consist of nothing more than fibrotic tissue. Postoperative course was good.
See pre and post op video

There are several disorders in young Rottweiler dogs that cause signs similar to those of this dog. Neuroaxonal dystrophy, leukoencephalomyelopathy, subarachnoid cyst and fibrotic stenosis all have been described in this breed. All three disorders will cause a progressive ataxia and hypermetria, especially in the thoracic limbs. Myelography and/or other imaging is helpful in revealing spinal cord compression. CSF examination may be helpful also. In both neuroaxonal dystrophy1and leukoencephalomyelopathy2the ancillary tests yield normal results. In these diseases, diagnoses must be made by necropsy and histological examination of the brain and spinal cord.
In an earlier report, Baum, de Lahunta, and Trotter3 described a young Rottweiler with a progressive cervical myelopathy. Their diagnostic testing, surgical findings and surgical biopsy report were similar to this case. The cause of the stenosis at this site in Rottweilers is still unknown. It is thought that ligamentous proliferation may be secondary to joint instability and chronic stress, but instability was not identified in the previous case report nor in this case.
References
1. Chrisman CL, Cork L, Gamble AD. Neuroaxonal dystrophy of Rottweiler dogs. J Am Vet Med Assoc 1984; Vol 184: 464-467.
2. Gamble AD, Chrisman C. A leukoencephalomyelopathy of Rottweiler Dogs. Vet Pathol 1984; 21:274-280.
3. Baum F, de Lahunta A, Trotter E J. Cervical fibrotic stenosis in a young Rottweiler. J Am Vet Med Assoc 1992; Vol 201: 1222-1224.
[Top]