Virginia Luis Fuentes, VetMB, PhD, CertVR, DVC, MRCVS, Diplomate ACVIM (Cardiology)

INTRODUCTION
Myocardial disease is common in cats. In human patients, cardiomyopathy has traditionally been classified into three basic primary ("idiopathic") forms: dilated cardiomyopathy (DCM), hypertrophic cardiomyopathy (HCM) and restrictive cardiomyopathy (RCM).1 Specific heart muscle diseases of known etiology were classified separately. This classification system was also used in feline myocardial disease, with an additional category of "intergrade"/ "intermediate" or "unclassified" cardiomyopathy for those patients difficult to categorize as one of the three basic forms. More recently, the distinction between primary cardiomyopathy and specific heart muscle diseases has become more blurred, both in people and in cats, as genetic or other causes have been found for primary cardiomyopathies (such as taurine deficiency in cats with DCM). The current accepted classification system for human myocardial disease acknowledges DCM, HCM, RCM, arrhythmogenic right ventricular cardiomyopathy (ARVC), and "unclassified" cardiomyopathies.2 This classification system has supplanted the old system in cats as well, although increasing overlap between categories is recognized. Pathological processes such as myocarditis and infarction may be occur in more than one type of cardiomyopathy, so that the original phenotype may not be obvious at the time of clinical presentation.
As well as occurring as a range of different disease types, cardiomyopathies may occur with a range of severity, from clinically insignificant disease to intractable heart failure and death. This means that diagnosis of feline cardiomyopathy can be potentially challenging for practitioners and cardiologists alike, although certain characteristics can be extremely useful in arriving at a diagnosis.
TYPES OF CARDIOMYOPATHY
The following descriptions are based on the most widely used classification of feline myocardial disease, although there may be some overlap between categories that can cause difficulties in labeling individual cases. It may be more important to recognize the type of functional disturbance (for example, predominantly systolic versus diastolic dysfunction) rather than to arrive at a precise categorization.
Hypertrophic cardiomyopathy (HCM)
HCM is the most common of feline myocardial diseases and also the form with the most varied phenotype. Most cases of human HCM appear to be associated with mutations in sarcomeric proteins; it is not yet known if the same is true in cats. In the absence of molecular markers for HCM in cats, the condition is defined as left ventricular hypertrophy without obvious cause (ie. not due to systemic hypertension, aortic stenosis or hyperthyroidism). Functionally, HCM is characterized by impaired ventricular relaxation and increased ventricular stiffness (diastolic dysfunction), which may impose problems with ventricular filling, leading to increased atrial pressures and congestive failure. A frequent associated finding is dynamic left ventricular outflow tract obstruction (LVOTO), generally caused by abnormal motion of the anterior mitral leaflet during systole, where the leaflet moves towards the outflow tract during ejection instead of co-apting normally. This dynamic obstruction may be intermittent or persistent. Other complications, such as myocardial infarction, may cause regional systolic dysfunction that may cause difficulties in recognizing the original phenotype as HCM.
Pathological findings
Hypertrophy of the left ventricle (LV) may affect both septum and free wall equally, or the septum or free wall preferentially. The papillary muscles may be markedly hypertrophied. The left (and right) atrium may be dilated when filling pressures are increased. The mitral valve leaflets may be thickened or abnormally long, with abnormal arrangement of the papillary muscles. Myocardial infarction may occur, appearing as localized wall thinning with scarring. Histologically, myofiber disarray may be noted within areas of LV hypertrophy, and myocardial fibrosis is common, especially in areas with abnormal small intramural coronary arteries.3 Myocarditis has also been noted in cats with HCM.4
Clinical presentation
Although the highest incidence of HCM may be in young adult male cats, the signalment can be very varied.5 It may be seen in kittens less than six months, as well as in cats over 10 years. Some breeds may be predisposed or have a familial form of HCM, such as Maine Coons, Persians, Ragdolls and Cornish rexes. Some cats with HCM are completely asymptomatic, and may not even demonstrate any abnormalities on physical examination, although other cats have murmurs or gallop sounds, and occasionally arrhythmias. Congestive heart failure when it occurs may be severe and acute, with life-threatening pulmonary edema. Pleural effusion may also occur. Cats with HCM are predisposed to thromboembolic disease.
Dilated cardiomyopathy (DCM)
The incidence of feline dilated cardiomyopathy has decreased in recent years, thanks to the discovery of the role of taurine in the etiology of DCM, and subsequent changes in the formulation of commercial feline diets.6 Although cats are still sometimes seen with taurine-deficiency DCM, most cats diagnosed with DCM nowadays have normal serum taurine levels. DCM is characterized by dilation of all four chambers, with thinning of the ventricular walls and hypokinesis (systolic dysfunction).
Pathological findings
In addition to dilation of all four chambers, the left ventricle is usually thin-walled and more spherical in shape than normal, with small papillary muscles.7 Attenuated wavy fibers may be seen on histopathology, with abnormal extracellular matrix architecture (loss of normal collagen weaves and struts).
Clinical presentation
Middleaged and older cats are typically most likely to develop DCM, with taurine-deficiency DCM mostly occurring in cats fed on dog food. Cats with dilated cardiomyopathy are rarely diagnosed while asymptomatic, and generally present with a varying combination of output failure and congestive signs. Poor cardiac output signs may predominate in some cats, so that they present with hypotension, hypothermia and bradycardia (essentially, cardiogenic shock) without marked fluid retention. Thromboembolic disease is common.
Restrictive cardiomyopathy (RCM)
Restrictive cardiomyopathy is characterized by severely impaired diastolic filling associated with increased ventricular stiffness, and relatively normal left ventricular dimensions and systolic function. Two main forms are recognized: an endomyocardial form, and a myocardial form.8 The endomyocardial form is associated with severe endomyocardial scarring, which may result in obliteration of the mid to distal portion of the left ventricular cavity and may even involve the mitral valve. The presence of inflammatory infiltrates may indicate the presence of endomyocarditis. The myocardial form may demonstrate more diffuse myocardial fibrosis. In both types, atrial dilation may be substantial. Mild LV hypertrophy may be present, but not to the extent of HCM. Mild systolic dysfunction may be present, but not to the extent of DCM.
Clinical presentation
Affected cats are generally older, and rarely diagnosed while asymptomatic. Biventricular congestive failure is usually present, and both arrhythmias and thromboembolic disease are common.
Arrhythmogenic right ventricular cardiomyopathy (ARVC)
This form of cardiomyopathy has only recently been recognized in cats, and is characterized by fibrofatty infiltration of the right ventricle, resulting in marked right heart enlargement.9 Affected cats may be asymptomatic, may be syncopal in association with arrhythmias, or may have right-sided heart failure.
APPROACH TO DIAGNOSIS OF MYOCARDIAL DISEASE
Myocardial disease must be differentiated from other types of cardiac disease, as well as non-cardiac disease. In some instances, a murmur may not be associated with any structural heart disease at all.
Differential diagnosis of myocardial disease according to presentation
|
Presentation |
Possible myocardial disease |
Other differentials |
|
Asymptomatic cat with murmur |
HCM
ARVC |
Functional murmur (anemia, high cardiac output, aortic dilation)
Hyperthyroidism
Systemic hypertension |
|
Dyspneic cat without murmur |
HCM & CHF
DCM & CHF
RCM & CHF
ARVC & CHF
|
Pleural effusions
Noncardiogenic pulmonary edema
Intrapulmonary hemorrhage
Asthma
Heartworm disease
Thromboembolism
Mediastinal masses
Pulmonary neoplasia
etc |
|
Dyspneic cat with murmur |
HCM & CHF
DCM & CHF
RCM & CHF
ARVC & CHF |
Congenital heart disease- AV valve dysplasia, VSD, PDA, AVSD & CHF
Hyperthyroidism & CHF
Anemia & CHF |
History
When signs of heart disease are detected in a cat presented for a routine health check, HCM is more likely than RCM or DCM, as the latter are generally symptomatic at the time of presentation. Presenting signs are sometimes vague, and may be as non-specific as lethargy, inappetence or even vomiting. Coughing is not typically seen with cardiac disease in cats. Cats with severe systolic dysfunction may present with profound weakness. It is not unusual for cats with myocardial disease to present with acute onset pain and limb paresis from thromboembolism (the owner usually assumes a traumatic cause in these cases).
Physical examination
In contrast with congenital heart disease, physical examination may be completely normal in some cats. Observation is very important in the assessment of respiratory difficulties, and cats with pulmonary edema or pleural effusion will have increased respiratory rate with inspiratory and expiratory effort, and no audible airway noise. In HCM, the apical impulse may be especially prominent. Jugular distension may be evident with right heart failure (or some noncardiac pleural effusions). Femoral pulses may be weak in any of the cardiomyopathies, or absent with aortic thromboembolism. Ascites is far less common than pleural effusion with congestive failure due to cardiomyopathy. Retinal degeneration may be seen in taurine-deficient cats.
Auscultation
Gallop sounds may be detected in all types of myocardial disease, and their presence is very suggestive of cardiomyopathy. Murmurs are highly variable, with the loudest murmurs typically found with HCM (although some HCM cats will have no murmurs). Intermittent murmurs (murmurs that vary in intensity with excitement) are suggestive of either HCM with LVOTO, or functional murmurs. Cats with DCM and RCM tend to have very soft holosystolic murmurs over the left or right sternal border (or may not have any audible murmur). Heart sounds may be soft or muffled by pleural or pericardial effusions. Arrhythmias may occur with any of the cardiomyopathies. Crackles may be heard with pulmonary edema.
Radiography
Asymptomatic HCM cats may have minimal changes on survey radiographs, especially if left atrial size is normal. The concentric hypertrophy may result in an elongation of the cardiac silhouette on lateral views, although apparently normal films do not conclusively distinguish between cats with mild HCM and cats with functional murmurs.
Figure 1A and 1B. Lateral and dorsoventral radiographs of a cat with HCM.
Note the increased apicobasilar length on both views, with left atrial enlargement evident on both views in this particular case. Shifting of the apex to the right hemithorax is not unusual. Click on image to see a larger view.
| Figure 1A | 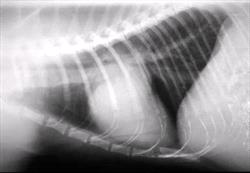
|
|
| |
| | Figure 1B | 
|
|
| |
|
Unfortunately, it is not possible to differentiate between the different forms of cardiomyopathy on the basis of radiographs. Cardiomegaly and biatrial enlargement may be seen with HCM, RCM and DCM. Pulmonary edema may be much patchier than in dogs, sometimes with alveolar infiltrates that appear granular. Pulmonary vessels (both arteries and veins) may be wide and tortuous, in contrast to heartworm disease where the arteries only may be abnormal.
Figure 2A and 2B. Lateral and dorsoventral radiographs of a cat with RCM and pericardial and pleural effusions.
Although the cardiac silhouette is difficult to see because of the pleural effusion, it is still possible to discern that the heart is much larger and rounder than normal, as a result of a large pericardial effusion. Cats with RCM and DCM will often develop pericardial effusions secondary to congestive heart failure. Click on image to see a larger view.
| Figure 2A | 
|
|
| |
| | Figure 2B | 
|
|
| |
|
Electrocardiography
ECG abnormalities may be seen in all forms of cardiomyopathy.8 A left anterior fascicular block pattern is particularly associated with HCM or hyperthyroidism, and may be found in asymptomatic as well as symptomatic HCM cats.
Figure 3. Left anterior fascicular block in a cat with HCM.
Typical features include a left axis deviation with a qR configuration in lead I, and deep S waves in leads II, III, and aVF.
Wide P waves may be seen with any cardiomyopathy when there is left atrial enlargement, and increased QRS voltages may also be seen with any form. Conversely, small voltages may be present whenever there are pleural or pericardial effusions. A variety of arrhythmias may be seen with any myocardial disease. Atrial arrhythmias may occur whenever there is severe atrial enlargement, and ventricular arrhythmias may be seen in all forms. First degree atrioventricular block may be particularly common with DCM.
Echocardiography
Although angiography has been used to obtain a definitive diagnosis in the past, echocardiography has become the diagnostic method of choice for differentiating between the different forms of myocardial disease, and ruling out functional murmurs. Two-dimensional echocardiography (2DE) is an excellent technique for demonstrating the morphological changes seen with the different forms of myocardial disease.
Although M-mode echocardiography has traditionally been used for measuring chamber dimensions, there are a number of limitations with its use in assessing feline cardiomyopathy. In mild HCM, hypertrophy may be localized to areas other than those crossed by the M-mode cursor, so that abnormal wall thickness may be missed. In severe HCM, it can be difficult to avoid crossing through the papillary muscles. In the endocardial form of RCM, it is difficult to obtain meaningful M-mode pictures because of the severe mid-ventricular scarring. Notwithstanding these limitations, M-mode can still be useful for demonstrating increased LV diameter and reduced systolic function (often assessed using the LV fractional shortening), and for identifying systolic anterior motion of the mitral valve in HCM. Left atrial (LA) size is also a very important measurement, and may be assessed by M-mode using the LA: aortic ratio (generally around 1.0).
Much more information can be obtained about morphology using 2DE. Doppler echocardiography provides further refinement in the assessment of LVOTO gradients, atrioventricular valve insufficiency, and diastolic function. Nevertheless, most of the diagnostic information can be obtained by 2DE.
Some controversy exists over the exact classification of cats that do not fall into the classical categories of feline myocardial disease. A typical example would be cats that have a combination of focal hypertrophy with regional systolic dysfunction, which might be classified as end-stage HCM by some, myocardial RCM by others, or unclassified cardiomyopathy or even DCM. Until more data are available on the underlying pathophysiological processes in these cats, it is probably prudent to confine descriptions to the predominant functional disturbance (ie. is systolic function normal or abnormal?). While different clinicians might give a different name to a disease in a particular cat, there is usually better agreement on which aspect of cardiac function appears to be perturbed following echocardiographic assessment.
HCM
Left ventricular hypertrophy is generally recognized when septal or free wall thickness exceeds 6 mm.10 The extent and location of hypertrophy in HCM may be extremely variable, and merits careful evaluation using multiple 2DE views, measuring the end-diastolic wall thickness directly from the 2DE image.10-12
LA size may indicate the degree of hemodynamic compromise, with LA size being greater in HCM cats dying with congestive failure than in HCM survivors in one study.10 Systolic function is usually normal to hyperdynamic, and LV diameter is usually normal to reduced. Demonstration of systolic anterior motion of the mitral valve can indicate the cause of a systolic murmur in cats with HCM and LVOTO. Subaortic stenosis should be ruled out as a cause of the LV hypertrophy, and not confused with small hyperechoic "kissing lesions" of the septum, where mitral-septal contact occurs in LVOTO.
Doppler echocardiography can be used to indicate the magnitude of the pressure gradient across the LV outflow tract in such cases, as well as demonstrating the degree of associated mitral regurgitation. Diastolic function can be assessed using a combination of mitral inflow velocity patterns, pulmonary venous flow velocities, and color M-mode LV flow propagation velocities, but there is no one characteristic pattern of filling.
Figure 4. Right parasternal long axis 2D echocardiographic view of cat with HCM.
The septal and free wall thickness is measured directly from the 2DE image, and exceeds 6 mm in diastole in both walls. The left atrium was not dilated in this cat.
Figure 5. Right parasternal long axis 2D echocardiographic view of cat with severe HCM.
This cat had severe concentric hypertrophy, and a very dilated left atrium (note the bowing of the interatrial septum). The left atrial diameter (LAD) measured at its widest point in a long axis view optimized for the left ventricular inflow tract is generally < 1.5-1.6cm.
Figure 6. Left ventricular M-mode of a cat with HCM, demonstrating systolic anterior motion (SAM) of the mitral valve.
The anterior mitral valve (MV) leaflet opens normally during diastole, and then moves again towards the interventricular septum (IVS) during systole (arrow). LVFW = left ventricular free wall.
Figure 7. Right parasternal long axis color flow Doppler image of cat with dynamic left ventricular outflow tract obstruction.
A turbulent flow pattern is seen in the left ventricular outflow tract, with a separate jet of mitral regurgitation (blue/green).
Figure 8. Spectral Doppler continuous wave recording of left ventricular outflow tract blood flow velocity showing dynamic obstruction.
Velocity (y axis)-time (x axis) graph of LV outflow tract velocity, showing an increase in late systole associated with systolic anterior motion of the mitral valve. Normal velocity would be < 1.5 m/s, and this increased velocity indicates a late systolic pressure gradient of approximately 64 mmHg.
RCM
The endomyocardial form of RCM is fairly distinctive, although images may be initially disorienting. The endomyocardial scarring is readily imaged, and usually associated with severe biatrial enlargement.
Some wall segments may be mildly hypertrophied, and systolic function is usually subjectively normal or only slightly reduced (obtaining an M-mode fractional shortening can be difficult). Doppler echocardiography may demonstrate systolic or diastolic mid-ventricular gradients. The myocardial form may be more challenging, as the LV may appear relatively normal but with a markedly dilated LA (± dilated RA). Mitral valve abnormalities should be ruled out as a cause of the atrial enlargement (mitral regurgitation is usually relatively mild in RCM). Pericardial effusion may be present as a result of right-sided heart failure.
The severe ventricular stiffness and high atrial pressures associated with both forms result in a characteristic "restrictive" filling pattern, where most of the filling of the LV occurs rapidly at the beginning of diastole, but then stops after abrupt deceleration because of poor LV distensibility. This pattern can be seen in HCM or DCM as well, but is virtually always seen with RCM.
Figure 9. Right parasternal long axis view of a cat with the endomyocardial form of RCM.
Note the dilated atria, and complicated scarring pattern within the mid to apical LV lumen.
Figure 10. Spectral Doppler mitral inflow patterns showing different diastolic filling patterns.
Normal diastolic filling consists of early rapid filling at the beginning of diastole ('E' wave), and another wave of transmitral flow associated with atrial contraction ('A' wave). Normally, most filling occurs at the beginning of diastole. When LV relaxation is delayed, filling is shifter towards the later part of diastole, with a consequently bigger A wave. When LA pressures are high and the LV is stiff (as in "restrictive filling"), early filling is enhanced (bigger E wave) but flow decelerates abruptly.
DCM
The dilation and increased sphericity of the LV is evident on 2DE, and the reduced systolic function can be assessed by M-mode (fractional shortening less than 30%, with an LV end-systolic diameter >12 mm). All four chambers may be dilated, or only the left heart.
Sometimes hypokinesis of the free wall or septum only is seen. Pericardial effusions are often present. Central jets of mitral regurgitation (and tricuspid regurgitation) are often seen with color flow Doppler echocardiography.
Figure 11 and 12. Right parasternal long axis view and LV M-mode of feline DCM.
The 2DE image shows the dilation and spherical shape of the LV. Both the end-diastolic LV diameter (LVDd) and end-systolic LV diameter (LVDs) are greatly increased, with the percentage change in LV diameter (LV fractional shortening) much less than the normal 30% or greater.
ARVC
Severe right ventricular and right atrial dilation are the hallmarks of ARVC. It can be difficult to recognize the RV wall thinning, and the tricuspid valve may be mistakenly considered abnormal, because the dilation distorts the normal architecture. Nevertheless, the presence of an abnormal trabecular pattern near the apex of the RV can give some clues. Tricuspid regurgitation is usually present.
Figure 13. Right parasternal long axis view of cat with ARVC.
Note the dramatic right heart enlargement, with a trabecular band seen near the apex of the right ventricle.
Other diagnostic tests
Systemic arterial blood pressure must be measured in cases of LV hypertrophy to rule out systemic hypertension as a cause. Thyroxine levels should also be measured in any middleaged or older cat. Necropsy is the ultimate way to establish a diagnosis, but obviously is not helpful in management of the individual patient.
SUMMARY
Establishing a diagnosis of feline cardiomyopathy can be challenging, and requires astute clinical skills. Unfortunately, echocardiography is required for a precise evaluation of the form of cardiomyopathy, although myocardial disease in general can be suspected with a high degree of certainty based on physical exam, electrocardiography and radiography. Echocardiography plays a crucial role in assessing function as well as morphology in feline cardiomyopathy, and although some controversy exists over specific nomenclature, echocardiography is invaluable in providing a functional assessment that will help guide therapy.
REFERENCES
1. WHO/ISFC task force. Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br Heart J 44:672-673,1980
2. Richardson P, McKenna W, Bristow M, Maisch B, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of Cardiomyopathies. Circulation 93:841-842,1996
3. Liu SK, Roberts WC, Maron BJ. Comparison of morphologic findings in spontaneously occurring hypertrophic cardiomyopathy in humans, cats and dogs. Am J Cardiol 72:944-951,1993
4. Meurs KM, Fox PR, Magnon AL, Liu S, et al. Molecular screening by polymerase chain reaction detects panleukopenia virus DNA in formalin-fixed hearts from cats with idiopathic cardiomyopathy and myocarditis, Cardiovascular Pathology 9:119-126, 2000
5. Atkins CE, Gallo AM, Kurzman ID, Cowen P. Risk factors, clinical signs, and survival in cats with a clinical diagnosis of idiopathic hypertrophic cardiomyopathy: 74 cases (1985-1989). J Am Vet Med Assoc 201:613-618, 1992
6. Pion PD, Kittleson MD, Rogers QR, Morris JG. Myocardial failure in cats associated with low plasma taurine: a reversible cardiomyopathy. Science 237:764-768, 1987
7. Van Vleet JF, Ferrans VJ, Weirich WE. Pathologic alterations in hypertrophic and congestive cardiomyopathy of cats. Am J Vet Res 41:2037-2048,1980
8. Fox PR. Feline cardiomyopathies, in Textbook of Canine and Feline Cardiology, principles and clinical practice, ed. Fox PR, Sisson D, and Moise NS, WB Saunders Company, Philadelphia p 621-678, 1999
9. Fox PR, Maron BJ, Basso C, Liu SK, et al. Spontaneously occurring arrhythmogenic right ventricular cardiomyopathy in the domestic cat : a new animal model similar to the human disease, Circulation 102:1863-1870, 2000
10. Fox PR, Liu SK, Maron BJ. Echocardiographic assessment of spontaneously occurring feline hypertrophic cardiomyopathy. An animal model of human disease. Circulation 92:2645-2651,1995
11. Peterson EN, Moise NS, Brown CA, Erb HN, et al. Heterogeneity of hypertrophy in feline hypertrophic heart disease. J Vet Intern Med 7:183-189, 1993
12. Bright M, Golden AL, Daniel GB. Feline hypertrophic cardiomyopathy: variations on a theme. J Small Anim Pract 33:266-274, 1992.