Introduction
Obesity is the number one nutritional disorder in pets in the western world. Twenty five percent of cats seen by veterinarians in the USA and Canada are overweight or obese. Just as in people, over-consumption of calories results in storage and is manifested as excessive body fat. In optimal condition, cats should carry 15-20% body fat.
It has been shown statistically that obesity is a risk factor for diabetes mellitus, skin problems, hepatic lipidosis, and lameness. A more general look at the consequences of obesity adds additional risks: hyperlipidemia, insulin resistance, glucose intolerance, feline lower urinary tract disease, anaesthetic complications, dyspnea, exercise intolerance, heat intolerance, impaired immune function, exacerbation of degenerative joint disorders and dermatological conditions.
Risk Factors
Mixed breed cats were found to be at higher risk for becoming overweight than purebreds. This might be genetic, but husbandry and awareness of the cat may play a role. Because we confine cats indoors, feed them highly palatable, calorie-dense diets which they do not have to work for, and leave them alone many hours a day, possibly resulting in boredom, our cats are prone to consuming too many calories.
Neutering has been shown to reduce the energy requirements (resting metabolic rate) of cats by 20-25%. A link has been suggested between weight and fat gain following gonadectomy and serum leptin levels. It has also been shown that increased leptin levels may contribute to the decreased insulin sensitivity seen in overweight cats. Further work indicates that insulin resistance and glucose intolerance develop in obese cats especially in males, which also have increased risk for developing diabetes mellitus.
It is important, therefore, that we counsel our clients to restrict the amount we feed our neutered cats and watch carefully for weight gain adjusting caloric intake accordingly. Ten extra pieces of an average formulation kibble/day above a cat's energy needs can result in a weight gain of one pound of body fat in one year!
Cats reach their adult weight at about 12 months of age. This can be used as a guide to determine if a cat is becoming overweight. The longer a cat is overweight, the greater the chance that one of the negative consequences of obesity will occur.
Uniquely Feline
What factors peculiar to cats do we need to consider when addressing obesity? Cats weren't designed to utilize carbohydrates. As obligate carnivores, they have a smaller stomach and shorter intestinal tract relative to their body size when compared to omnivores or herbivores. This is a reflection of their need for frequent meals.
Their normal diet of small prey provides them with protein and fat. Cats lack salivary amylase and have only 5% of the pancreatic amylase activity and 10% of intestinal amylase activity of dogs. Cats derive less energy per gram of carbohydrate than humans or dogs do. Cats have a vestigial cecum and a short colon which limits their ability to use poorly digestible starches and fibers through microbial fermentation.
This does not, however, imply that cats cannot use carbohydrates. They can use carbohydrates quite efficiently despite lacking a dietary requirement for them. Carbohydrates are a good energy source and have been shown to be necessary for lactating queens. If there is too much lactose or other sugars in the diet, then bloating, diarrhea and flatulence may result.
These points may be of clinical significance when considering the role that dry formulations (which contain more carbohydrate than other formulations) play in the way we feed cats. We really don't know what impact long term carbohydrate intake plays in predisposing cats to obesity and diabetes mellitus. Research is ongoing.
Assessing Body Composition
It is easier to prevent weight gain than to lose weight. The prevalence of obesity increases after two years of age, plateaus until about 12 years and then declines thereafter.
What tools do we have to help prevent the development of obesity? At every veterinary visit, determining and recording the patient's body weight and calculating the percent weight change is invaluable for the detection of weight change patterns. Many a cat with early chronic illness has been identified using this calculation:
% weight change = (current weight - previous weight) / previous weight.
Use a body condition scale (BCS) at every visit, categorizing the body condition as emaciated, thin, ideal, heavy or grossly obese (1-9 or 1-5 scale). In ideal condition, the bony prominences of the body (i.e., pelvis, ribs) can be readily palpated but not seen or felt above skin surfaces. There should be insufficient intra-abdominal fat to obscure or interfere with abdominal palpation. In questionable cases, radiographs and ultrasound may be used to assess falciform, paralumbar and perirenal fat. In research settings, dual energy X-ray absorptiometry (DEXA) evaluation is used for the most accurate bone density, muscle mass and fat calculations.
What to Feed
Simply feeding less of a normal diet is not recommended. Not only will the patient be unhappy and feel hungry, but nutritional balance will be compromised. A diet should be balanced according to energy content. When a cat eats enough of the diet to meet energy requirements, their protein, vitamin and mineral needs will be met as well. An energy-limiting diet is one which is so energy dense that a cat will stop eating once energy needs have been met, but before protein and other nutrient needs have been met. Similarly, a bulk-limiting diet will cause the individual to stop eating before energy and other nutrient needs have been met.
In cats, meeting protein needs as well as energy needs induces satiety. During weight loss, feeding a protein replete diet will help protect against loss of lean muscle mass. For safe weight loss, cats need >35% crude protein (dry matter basis), < 3.6 kcal metabolizable energy (DM), as well as 7-14% fat (DM).
When discussing with clients why reduced quantities of normal foods won't result in successful weight loss, the following may be considered:
 Normal diets are too high in fat.
Normal diets are too high in fat.
Fat is an easy energy source for manufacturing.
There is less thermic energy formed in the digestion of fat.
Digestibility is inversely proportional to the amount fed.
All nutrients are decreased when you feed less of a balanced diet.
An individual's energy requirements are composed of several components.
The daily energy requirement (DER) = resting energy requirement
 + exercise energy requirement
+ exercise energy requirement
+ thermic effect of food (TEF)
+ adaptive thermogenesis (AT)
Resting energy requirement varies with individuals; this accounts for the apparently higher manufacturer recommendations vs. a given individual's food needs.
TEF is the energy spent on digesting and absorbing food. Increasing the frequency of meals and decreasing their size results in an increased TEF expenditure. AT is the energy used to regulate body temperature. DER decreases with increasing age.
A Clinic Weight Loss Program
In order to be successful with any weight loss program, three components must be in place: diet, exercise and recheck visits. Without any of these, the client's desire for their cat to slim down will fail. A diet alone can't do it; recheck visits monitor progress and provide support. We need to reduce the number of calories consumed, and increase calorie use and metabolic rate (exercise). Exercising cats could be seen as an oxymoron, however, some dedicated clients have even designed agility obstacle courses for their cats. Their commitment is the fuel for the success of the program.
On the initial extended consultation, a comprehensive physical exam is performed to rule-out concurrent medical problems. Baseline blood work may be advisable, depending on the cat's age and condition. A detailed history is collected in order to become familiar with current feeding habits and routines. Table 1 contains useful questions for this purpose.
Counsel the client to start a one-two week journal in which everyone in the household who gives the cat anything ingestible, enters the information. The amount of food as well as exact type (brand) should be recorded. From this the caloric content leading to the weight gain can be determined. As a rule of thumb, in order to lose weight, a cat needs 60-70% of the calories required to maintain his/her ideal weight. In other words:
1. Determine/approximate ideal weight
2. Calculate calories needed for ideal weight (wt in kg X kcal/kg/day)
3. Multiply this number by 60-70% (may need to use 50% if very inactive)
Discuss with the client the benefits of weight loss and the risks of chronic obesity. Acknowledge them for their concern and praise them for their desire to take action. Be supportive! They are the ones who will have to do the work!
Inform them of the current weight as well as the goal weight, vs. the 'ideal' weight. Discuss with them the length of time this may take. A safe rate of weight loss is 1/4-1/2 pound/month (0.1-0.25 kg/month). This will help them stay on track.
As mentioned above, the TEF is higher when small frequent meals are fed, so feeding multiple small meals is preferable to feeding one or two large meals. One way to incorporate this with exercise is to divide the day's food amount on to 6 or 7 small saucers and place them throughout the home as if it were a 'treasure hunt'. This means that kitty is less likely to gorge, has to look for more and has a higher TEF cost.
Discuss with the client why cats become overweight. Pet food manufacturers have to make diets extremely palatable, because that is how a consumer judges how much their companion likes it and decides whether to buy it again or not. This means that most cat foods are very energy-dense from fat, as fat is palatable for cats. In addition, because it is convenient to feed ad libitum, cats snack all day on high calorie kibble, and easily eat more than they need. Cats generally lack exercise, when compared to the hunter that they are designed as. In the wild, they have to catch 10 small meals a day to survive! An indoor environment is not very stimulating; cats may eat out of boredom. Former strays may also have the fear-driven instinct to gorge in case there isn't another meal.
The behaviour modification required to make a weight loss program successful, needs all key family members to play a role. Treats are the downfall of many a weight control program. It is best if one person handles all of the feeding and others bond through other means (catnip, combing, playing). Developing a routine of playing with a 'cat dancer' (a hand held flexible wire with a toy on the end) several times a day will add interest and exercise. Send home a 'weight loss pack' with food samples (dry and canned) for kitty to choose from.
Create a bar graph to maintain in the clinic computer and kitty's medical record (Figure 1). Update and send the updated graph home with the client at every visit as a reminder of their success.
| Figure 1. Weight loss graph. | 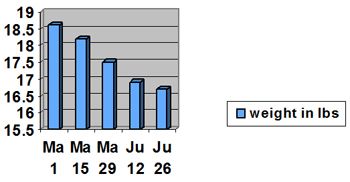
|
|
| |
No weight loss program is effective without follow-up! A technician or nurse should become the client's 'buddy' and be in charge of the follow-up:
Week 1: support phone call
Week 2: 15 minute visit with program supervisor and veterinarian:
Weigh in
Conversation about highlights, problems
Update graph
Every 2 weeks come in for weigh-in
Update and send home graph
After 4 months, a 15-minute visit with the supervisor is advisable because plateauing may occur, and new calculations may be needed to promote further safe weight loss
Included in the program cost is unlimited buddy phone support. The program lasts 6 months and is renewable if necessary.
Table 1. Questions for diet history.
Diet History
Amounts and type of food (all, including treats)
Milk?
People food?
Hunting?
Who feeds the cat?
Frequency of feeding?
How is food measured?
Medications?
How are medications given? In food or with a treat?
Does cat nibble or gorge?
What other pets are there in the home?
Do other pets have access to this food?
Does this cat have access to their food?
Where is cat fed?
Is there any known stress?
Activity level?