Kenneth W. Simpson, BVM&S, PhD, DACVIM, DECVIM-CA
Introduction
Esophagitis has been associated with the ingestion of chemical irritants, thermal injury, gastroesophageal reflux (GER), hiatal hernia, foreign body ingestion, viral infection and persistent vomiting.
Medications such as doxycycline, tetracycline, potassium chloride and acetyl salicylic acid may increase the risk of esophagitis.
A small amount of GER is a normal phenomenon in dogs and cats. Appropriate lower esophageal sphincter tone, esophageal peristalsis and intact esophageal mucosa limit and minimise the effect of acid reflux. Disruption of the LES, esophageal peristalsis or the esophageal mucosa increase the risk of esophagitis secondary to acid reflux. The effect of acid reflux on the esophagus depends on the frequency of reflux, the acidity of gastric contents and the duration of contact of acid with the esophagus. While esophagitis is the initial consequence of exposure of the esophagus to gastric acid, esophageal dilatation (megaesophagus), perforation and stricture formation may also occur. Recumbency and anesthesia may increase the risk of GER and have been associated with esophagitis and esophageal stricture formation. Zollinger-Ellison syndrome, which is characterized by massive hypersecretion of gastric acid, has also been associated with esophagitis and esophageal perforation. Shar peis appear to have a high incidence of hiatal hernia.
The clinical signs of esophagitis include: anorexia, painful swallowing, hypersalivation and regurgitation.
Treating the underlying cause (e.g., hiatal hernia), decreasing gastric acid secretion, providing a diffusion barrier against gastric acid, increasing lower esophageal sphincter (LES) tone to prevent reflux and decreasing vomiting with antiemetics / prokinetics are the main ways of managing esophagitis.
Decreasing Gastric Acid Secretion
The regulation of gastric acid secretion is summarized in Figure 1. Acetylcholine and GRP stimulate gastrin secretion from G cells which effects histamine release from ECL cells. Histamine is also released from mast cells. Acetylcholine and gastrin can also directly stimulate acid secretion. Somatostatin acts to decrease gastrin, histamine and acid secretion.
Acid secretion can be decreased by blocking H2 (cimetidine, ranitidine, famotidine), gastrin (proglumide) and ACh (atropine) receptors and by inhibiting adenyl cyclase (PGE analogs) and H+/K+ ATPase (e.g., omeprazole) (Table 1). Somatostatin directly decreases gastric acid secretion and gastrin secretion.
Click on the image to see a larger view.
| Figure 1. Regulation of acid secretion. | 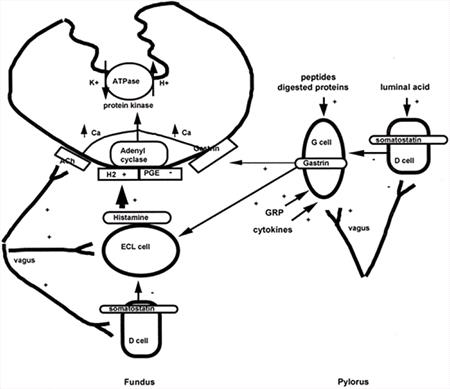
|
|
| |
Author's diagram published in: Dibartola: Fluid Therapy in Small Animal Practice 2nd Ed, Saunders.
Choice of Antisecretory Agent
H2-Receptor Antagonists
These are widely available and relatively inexpensive and potent. Potency: famotidine > ranitidine > cimetidine. Cimetidine can inhibit the hepatic P450 system and may enhance serum cisapride concentrations. Ranitidine and famotidine do not significantly inhibit P450 system. Rantidine has a prokinetic effect. Famotidine can be administered once per day.
H+/K+ ATPase Inhibitors
E.g., omeprazole. Extremely potent, twice per day administration to dogs. Affects P450 system and may prolong half life of diazepam, warfarin and phenytoin. Used when maximal acid suppression is required and when therapy with H2-receptor antagonists is unsuccessful, e.g., in patients with severe esophagitis and excessive acid secretion secondary to mast cell tumors and Zollinger-Ellison syndrome. Omeprazole should be used with particular caution in patients with liver disease.
Somatostatin Analogs
E.g., octreotide. Very potent inhibitor of gastric acid secretion. Expense and parenteral dosing have limited its clinical application to patients with ZES. Hypoglycemia is a potential side effect.
Diffusion Barriers
Diffusion barriers, e.g., Sucralfate (polyaluminum sucrose sulfate), are used to protect the esophageal and gastric mucosa where ulcerated or eroded (Table 1). It may compromise absorption of other drugs if given simultaneously. Often used in association with antacids in patients with gastric erosion/ulceration and as a slurry in patients with esophagitis.
Table 1. Therapeutic agents used to decrease acid secretion or act as a diffusion barrier.
|
Drug name |
Suggested dosage |
|
Famotidine (Pepcid) |
0.5-1.0 mg/kg PO S-BID |
|
Omeprazole (Prilosec) |
0.7 mg /kg PO BID |
|
Octreotide (Sandostatin) |
2-16 µg / kg SC TID |
|
Sucralfate (Carafate) |
0.25-1 g PO TID |
Increasing LES Tone
Cisapride and metoclopramide have been demonstrated to increase LES tone in dogs (Table 2). Little information is available regarding the clinical efficacy of these agents in dogs and cats with esophagitis or GER. They may be used alone or in combination with acid reducing agents and diffusion barriers in patients with esophagitis. These agents delay esophageal transit, thus their potential impact on esophageal transit versus gastric reflux has to be weighed up.
Table 2. Therapeutic agents used to increase LES.
|
Drug name |
Suggested dosage |
|
Metoclopramide |
0.25-0.5 mg/kg PO T-QID |
|
Cisapride |
0.1-0.5mg/kg PO B-TID |
Anti-emetics
Antiemetics are often used in patients with concurrent vomiting and esophagitis / high risk for oesophagitis or aspiration pneumonia.