Test Yourself--A First Assessment of the Dog Bite Prevention Project "Blue Dog". Part I: Education--The "Blue Dog" is Born; Part II: The "Blue Dog"--Do Children Really Get the Message?
Introduction
The majority of dog bite accidents happen at home and involve younger children. In the majority of accidents (86%), a child's interaction with a familiar dog appears to trigger the biting (Kahn et al. 2003). The prevalence of dog bites in children is 2,2 % which is double as in the general population (Kahn et al. 2004 ) and often, children suffer from dog bites resulting in facial injuries (Bernardo et al. 2002, Kahn et al. 2003, Schalomon et al. 2006). 55% children suffer post-traumatic stress disorder following a substantial bite (Peters et al. 2004). Dog bite prevention programmes exist mainly for children aged 7 years and older (Chapman et al. 2000) and mainly focus on public safety rules, like how to behave when encountering an unfamiliar dog. Only very few programmes are aimed at children under 7 and intend to prevent bite accidents at home (British Kennel Club 2004, Jung et al. 2001; ONE 2003, Pillonel, 2003).
However, as children who are bitten are five years on average, the authors attempted to remedy the lack of early prevention programmes--our aim was to empirically assess if children can learn from a CD; we used a specially selected and adapted subset of the Blue Dog interactive prevention scenes. The Blue Dog project targets children under the age of 7 and uses an interactive CD to tell children about an abstract "Blue Dog" and to teach them via the character of the Blue Dog about safe and unsafe interactions with a dog. The CD also includes a "Test Yourself" module, which is the part that has been used for assessment of the CD's effect on children's learning. This module has been shown to teach children successfully about safe and unsafe behaviour with dogs in a home context.
Method
Participants: Children were tested at 3, 4, 5 and 6 years of age. Testing of children's progress in learning was carried out in schools in Lincolnshire, UK, with 3-year-olds being tested using the interactive CD in nursery schools. 3-year-olds were also tested using Intermodal Preferential Looking (IPL; method used as in improved adaptation, see Meints et al. 1999)--a method that is frequently used in developmental psychology, for example in word learning and which does not require the children to interact with the experimenter, the laptop keys etc., but relies solely on infants' looking preferences.
IPL was used in the purpose-built Infant Lab at the University of Lincoln, UK, as 3-year-olds' ability to use a laptop successfully was more limited. About 26 children per age group per setting were tested.
Materials
The interactive learn and test CD module was created from the existing Blue Dog CD (De Keuster et al. 2005) that is usable for children from as early as 3 years of age.
The clips were condensed to 8 different 10-second clips with varying, in real-life frequently occurring situations (e.g., dog eating, dog sleeping, etc.) which children need to learn to react to appropriately.
Procedure
All children were shown three different experimental phases (each containing the 8 clips). They were first exposed to the stimulus videos, (exposure phase), then trained how to distinguish safe from unsafe situations (training phase) and finally tested on what they have learned (testing phases 1 and 2).
More specifically, in the 8 exposure trials, children saw see a child and dog interacting up until a point in time when the child has to choose an outcome. The child is free to choose any outcome. Then, the training phase began in which children were shown a possible negative (dangerous) and positive (safe) outcome of each child-dog-interaction. Half the children received additional, pre-recorded verbal feedback. Finally, in the first test phase, children saw the initial 8 scenes again straight after the training phase, but with different dogs and children. They were asked to choose the interaction that leads to a safe outcome. The second test phase took place in the same way, but with a two week delay. In the meantime, half of the children had received parental feedback, (half of these had received verbal input as well). Learning with parental reinforcement included looking at the story again at home with parents explaining / giving feedback. For IPL, eye-gaze direction was recorded on video and measured afterwards offline. For assessment via laptop children's button press choices were recorded.
Results
Results show a main effect of learning (F(2,184)=85.03; p< .0001) between the first exposure phase and the test phases. Results further show a main effect of age with older children exhibiting more correct responses than younger children (F(3,92)=6.23; p< .0007). Figure 1 demonstrates the increase in correct responses with age over the different testing phases.
| Figure 1. | 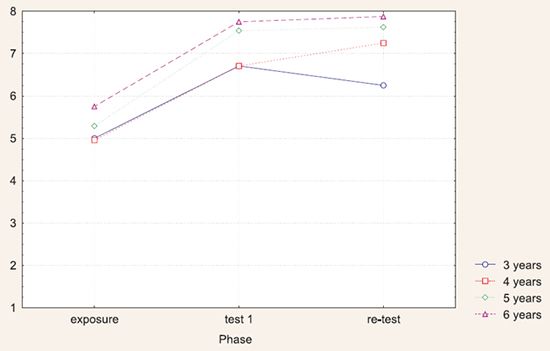
Mean scores of total correct answers as a function of phase and age. |
|
| |
There was also a significant main effect of parental input (F(1,94)=13.29; p< .0004) that demonstrated that children who received parental input performed better than those who did not receive parental feedback. More specifically, those children who received parental input seem to retain their acquired knowledge better than those without parental feedback as there is a significant difference in the first and second test phase with children supported by their parents performing significantly better than the control group (p< .0001). Figure 2 illustrates this result.
| Figure 2. | 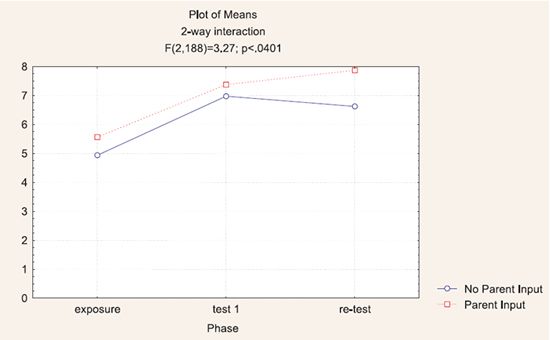
Mean scores of total correct answers as a function of phase and parental input. |
|
| |
While older children did not exhibit improvement via verbal, pre-recorded feedback, 3-year-olds, however, show a marked improvement in retaining their knowledge if they have received additional verbal feedback while watching the CD.
Discussion
The results of this first assessment indicate that children do indeed learn from the specifically adapted "Test yourself" module on the Blue Dog CD. Future research will have to show whether this learning is transferred not only to other dogs and children seen on a CD, but also to real child-dog-interactions. It will further have to be assessed whether the overall Blue Dog story can act as a learning facilitator by itself. In addition, as the role of parental feedback plays a role, further research will need to show the nature of this feedback and the best conditions and learning/teaching/feedback mechanisms for improving children's safety. As not all parents have access to computers, other forms of feedback should also be investigated and tested in a systematic way. The effectiveness and long-term impact of the learning should be tested as well (e.g., duration of retaining knowledge).
Conclusion
Overall, this first assessment of the effects of a CD aimed at improving children's understanding of safe and unsafe behaviour with dogs learning has successfully shown that children from 3 to 6 years are able to apply the acquired knowledge, even after a delay of two weeks.
References
1. Bernardo L, Gardner M, Rosenfield R, Cohen B, Pitetti R (2002) A comparison of dog bite injuries in younger and older children treated in a pediatric emergency department. Pediatr Emerg care 2002 Jun; 18(3): 247-249.
2. British Kennel Club--Safe and Sound
3. Chapman S , Cornwall J, Righetti J, Sung L: Preventing Dog Bites in Children (2000): Randomised Controlled Trial of an Educational Intervention. BMJ 2000, 320: 1512-1513.
4. De Keuster T, Moons C, De Cock I (2005) Dog bite prevention--How a Blue dog can help. EJCAP Vol 15; 2: 137-139
5. Jung H., Falbesaner U and Döring-Schätzl D. (2001) Grundwissen Gefahrenvermeidung im Umgang mit Hunden, Ed. Bayrische Landestierärztekammer und Institut für Tierschutz, Verhaltenskunde und Tierhygiëne , Universität München, ISBN 3-934302-05-x.
6. Kahn A, Bauche P, Lamoureux J and the Members of the Dog Bites Research Team (2003): Child victims of dog bites treated in emergency departments. European J Pediatr 2003; 162: 254-258.
7. Kahn A, Robert E, Piette D, De Keuster T, Lamoureux J, LevêqueA (2004) Prevalence of dog bites in children. A telephone survey. European J Pediatr 2004; 163: 424.
8. Meints K, Plunkett K, Harris PL (1999) When does an ostrich become a bird? The role of typicality in early word comprehension. Developmental psychology, 1999 Jul ; 35(4): 1072-8.
9. ONE (Office de la Naissance et de l'Enfance) http://www.one.be/home.htm
10. Peters V, Sottiaux M, Appelboom J, Kahn A (2004) Posttraumatic stress disorder after dog bites in children. J Pediatr 2004 Jan; 144 (1): 17-22.
11. Pilonell C., BVET: "Milou viens" http://www.bvet.admin.ch/index.html?lang=fr
12. Schalomon J, Ainoedhofer H, Singer G, Petnehazy T, Mayr J, Kiss K, Hollwarth M (2006): Analysis of dog bites in children who are younger than 17 years. J Pediatr 2006 Mar; 117 (3) pp 374-379.