MVZ Esp. MCP y G . Javier Del Angel Caraza
Hospital Veterinario para Pequeñas Especies, Facultad de Medicina Veterinaria y Zootecnia, Universidad Autónoma del Estado de Méx
More mistakes are made because of the lack of an appropriate exam, than for any other reason. Russel J. Howarc
Introduction
The normal urine of the dogs and cats is a complex solution that allows mineral salts to be kept dissolved under oversaturation conditions. Nevertheless, the oversaturated urine has a great potential of precipitation favoring the formation of solids (crystals) from the dissolved salts, with more oversaturation more crystallization potential.
The crystalluria is a consequence of the oversaturation with regard to the mineral or compound that precipitates. The grade of oversaturation necessary for the precipitation of a mineral is specific for each of these and at the same time, it changes according to the transitory physical and chemical conditions that exist in the urine. The principal factors that influence the mineral precipitation in the urine are: pH, temperature, the presence of certain compounds that act like as precipitation inhibitors, organic compounds like dead cells, cellular debris, proteins, bacteria or other crystals that act as precipitation promoters. The crystalluria is slightly common in dogs and cats, it does not bring problems for itself until an impediment exists in order that the crystals go out freely of the urinary tract or a massive production of the same ones exists.
In the majority of the cases in dogs, great relation exists with urinary pH alterations, due to a possible infection of the urinary low tract caused by some specific bacteria; in some dogs and in the majority of the cats it is due to abnormalities in the absorption or elimination of mineral compounds, consumption of acidification diets or genetic abnormalities that involve the metabolism and the elimination of metabolic final products.
If a sufficient number of crystals are formed and they adhere to the uroepithelium or remain caught inside the urinary tract instead of continuing their way as microscopic particles, it can form aggregations giving place to bigger particles big that finally originate a urinary calculus (urolith).
The uroliths damage the urinary tract mucous, which generates inflammation (hematuria, pollakiuria, dysuria, stranguria) and it predisposes to the bacterial colonization and infection of urinary tract. If the uroliths lodge at the ureters or urethra a post renal azotemia and uremic syndrome can occur in some cases. In studies realized by different universities of developed countries, has determined that in the majority of the cases the uroliths lodge at the urinary bladder or the urethra, and only 5 to 10 % at the kidney or the ureter. Being more frequent in dogs from 3 to 7 years.
PHYSIOPATHOLOGY
Of general form three principal theories have been proposed to explain the physiopathology of the urolithiasis: Precipitation-crystallization theory, Nucleation hypothesis, Crystallization inhibition theory.
Whichever the theory involved in the physiopathology, an important condition that must fulfill the urine is the unstable oversaturation (See picture 1). The urine must be oversaturated with minerals and these have to rely on suitable physical y chemical conditions that should facilitate the precipitation, like are the pH, temperature, etc. depending on the type of mineral.
| Picture 1. | 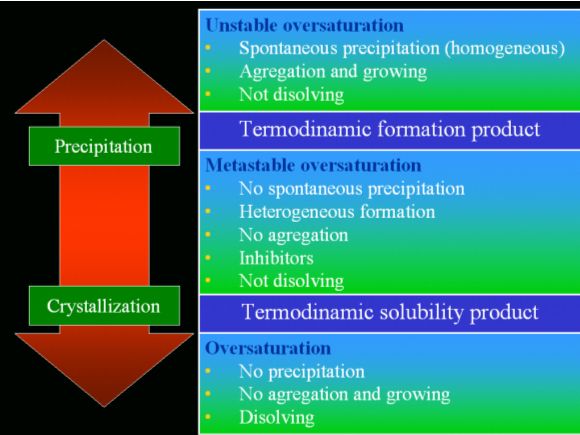
The normal urine is in a status of metastable oversaturation, there can be different types of crystals present depending on the diet, hour of the day, etc. they do not dissolve and nevertheless they do not add, that allows to expel them from the urinary route with the normal urination. The urolithiasis presents in the unstable oversaturation where a spontaneous precipitation exists and only an alone mineral precipitates, the crystals does not dissolve and they add together what prevents in occasions from eliminating them of the urinary route allowing the growth of the urolith. |
|
| |
Urolithiasis diagnostic
The clinical signs depend on the anatomical location, antiquity and physical characteristics of the uroliths precedents from the urethral acute partial or complete obstruction or signs of inflammation or infection of the urinary tract. The palpation of uroliths inside the urinary bladder, the presence of two or more shocking one against the other inside the bladder during the palpation, or by rectal exploration obstructing the pelvic urethra; the patients with uroliths in the unilateral renal pelvis can be asymptomatic or present hematuria and to develop pyelonephritis and can cause chronic renal insufficiency. Those who lodge at the ureters also can be asymptomatic or to present hematuria and abdominal pain causing often hydronephrosis.
The assessment of uroliths presence is done by simple radiographic studies or with contrast. The diagnosis of urolithiasis by ultrasonography is confirmed on having observed acoustic shades, in addition of having other advantages as that of being able to evaluate the architecture of the parenchymal structures and to differentiate with more precision soft tissues from liquids.
The urinalysis is a useful tool for the diagnosis of crystalluria, to determine the type of mineral that saturates the urine and represents part of the composition of the urolith; the determination of the pH is important for differential diagnosis of the uroliths, as well as some other general finds as, hematuria or pyuria, etc.
Another type of studies that can be of vital importance are the biochemical profile and CBC that will allow us to possess a general evaluation of the patient.
Removing the urolith, are we resolving the problem?
The general treatment only serves us to control the clinical signs of the urolithiasis and the ideal thing, is to withdraw the uroliths of the urinary route with the most common skill that is the surgery or any other skill and as soon as the uroliths are obtained, it is necessary to send them to the laboratory to determine their chemical quantitative composition and to be able to determine which is the medical handling adequate to avoid the problem recurrence.
"If a patient forms a urolith, the more probable is that it will form again; if a preventive medical management is not done"
Urinary Calculus analysis
It has been published the typical descriptions of size, shape, color and texture for the diverse uroliths (see Figure 1). Nevertheless, the macroscopic morphology is too diverse as for to allow a diagnosis based on the physical aspect. Besides, many uroliths are composed by two or more substances arranged in several layers, principally in the dogs. It is necessary to carry out a correct analysis of each one of them to determine the types of mineral that they are constituted. The majority of the dogs and cats that form uroliths from metabolic origin, as soon as they did it, they will do it again until a preventive treatment begins.
| Figure 1. | 
Notice the diversity of forms that the uroliths can have. Which can contain an alone type or several minerals independent of their shape. |
|
| |
Some other very useful methods exist to determine the mineral composition of the uroliths as: optical crystallography by oil dip with a polarized light, difractometry of X-rays, electronic microscopy, high pressure liquid chromatography, infrared spectroscopy, nevertheless, we have little experience with the use of these methods in the daily practice of our country.
The only available skill of commercial form in Mexico, to determine the mineral composition of an urolith is the mineral chemical semiquantitative analysis that allows us to determine the percentage of mineral compounds as phosphate, ammonium, magnesium, calcium, oxalate, urate, carbonate and cystine that can form the urolith. As a general rule, is important to send all the uroliths that are extracted from the urinary tract for their analysis.
Once having the report, it is necessary to analyze the percentages of components to determine the composition of the urolith. If a urolith has 80% of a mineral it is named from this mineral, if it is minor to 80% it will be mixed. For example:
|
Carbonate: |
Negative |
|
Calcium: |
40 % |
|
Oxalate: |
50 % |
|
Ammonium: |
1 % |
|
Phosphate: |
6 % |
|
Magnesium: |
3 % |
|
Urate: |
Negative |
|
Cystine: |
Negative |
The sum of the calcium with the oxalate gives me 90% and the ammonium, phosphate and magnesium only 10% those indicate me that the urolith is of calcium oxalate and very probably it presents an external layer of struvite.
|
Carbonate: |
Negative |
|
Calcium: |
20 % |
|
Oxalate: |
30 % |
|
Ammonium: |
10 % |
|
Phosphate: |
20 % |
|
Magnesium: |
20 % |
|
Urate: |
Negative |
|
Cystine: |
Negative |
In this case the calcium oxalate adds 50% and the struvite (phosphate, ammonium and magnesium) 50% which it indicates me that the urolith is mixed. Here we meet a dilemma: who is precipitating first, the calcium oxalate or the struvite? For what is necessary to combine other information of the urinalysis as the pH and urinary sediment, results from the uroculture and the clinic history.
If the pH is alkaline, in the majority of the cases we have an infection by urease unfolding bacteria and if some dietetic change history does not exist, the more probable is that the mineral that precipitates first is the calcium oxalate and secondarily the struvite due to the infection of urinary tract for bacteria because of the alteration in the defense mechanisms of the urinary tract. If the patient does not have signs of infection, an urinary acid pH and has received the medical handling with veterinary diets for urolithiasis, the most probable thing is that this patient has the facility to precipitate both minerals quite depending on the physical and chemical conditions in the urine, that in this case, the diet is acidifying the urine which facilitates the precipitation of the calcium oxalate.
There exist many types of minerals that can manage to form uroliths, nevertheless, the most common are those of struvite, calcium oxalate and urate for what is of supreme importance that the clinician knows the physiopathology of every mineral that precipitates. Remember that a urolith can be pure or mixed and only a stone analysis, along with other clinical information can help us to reach a precise diagnosis of which is the mineral or minerals that the primary problem is originating and based on this, to determine the most adapted handling to prevent the return urolith forming.
Brief summary of the physiopathology and the specific medical handling to avoid the recurrence of the principal types of uroliths
Struvite uroliths
They are of the most common uroliths in dogs and cats. In the majority of the cases of dogs 90%, the formation of the urolith is secondary to urinary tract infection with urease producing bacteria as the Staphylococcus intermedius, Proteus or Streptococcus; and in 10% of the cases they can be formed by sterile form. Due to the narrow relationship with the infection of the urinary tract, they are more frequent in the females and puppies younger than 5 months. The pathogeny of the struvite crystals in sterile urine of dogs is unknown; it is suggested that it stems from shortcomings of urine acidification on part of the kidney or tendency to form a highly concentrated urine, the last one is the principal cause of formation of struvite uroliths in the cats (more than 50% of the cases presents in sterile urine), which owes to the hyperosmolarity of the urine and because of this, a major grade of urine oversaturation.
To avoid the recurrence of these uroliths it is necessary to avoid the oversaturation of the urine based on a diet and increase in the water consumption. In general form, the diets designed for the urolith handling, avoid the oversaturation of the urine with phosphate, ammonium and magnesium. Provoking a oversaturation of the urine with these minerals, a major urinary volume and acidifying the pH and this way avoiding the crystallization and formation of uroliths. It is indispensable to increase the water consumption. (The diet by itself favors the increase of water consumption, nevertheless, in the cats it can be necessary to add little tuna water to the drinking water to make it more palatable). To control the infection of the urinary tract and the causes that provoke it in the specific cases.
Calcium oxalate
The majority of the information relating to this problem is an extrapolation of the information of human medicine, since it is in this specie where the biggest number of cases are observed. It is not a specific pathology, but the consequence of a series of underlying disorders that determine the precipitation of calcium oxalate in the urine.
The oversaturation of the urine by calcium and oxalate united to an acid pH and hypocitraturia, are conditions necessary for calcium oxalate urolith formation. The homeostasis of the calcium owes principally to the action of the parathormone and the cholecalciferol on the bones, the intestine and the kidneys. The hypercalciuria can be the result of an increase of the renal calcium excretion due to: (1) An excessive intestinal absorption, (2) an alteration in the renal calcium conservation, and (3) an excessive skeletal calcium reabsorption. The oxalic acid is the final product of the ascorbic acid metabolism and of some amino acids derived from the diet and from the endogenous synthesis. Forms soluble salts in sodium and potassium but relatively insoluble in calcium. The increase of the concentrations of oxalate in the urine facilitates the formation of calcium oxalate uroliths, rather than the increase of the urinary calcium concentrations. In the human specie it is related to hereditary disorders characterized by an excessive synthesis of oxalate (hyperoxaluria would occupy first place), with increase in the consumption of food rich in oxalate (ex. vegetables, grass or vitamin C) or its precursors, with shortcomings of piridoxine and with disorders associated with the bad fats absorption. The hyperoxaluria still has not been demonstrated in dogs with calcium oxalate urolithiasis due to the lack of a method for the determination of the urinary oxalate concentrations.
The hypocitraturia, is a physiological frequent disorder in these cases. The urinary citrate acts as an inhibitor of the calcium oxalate uroliths formation on having reduced the quantity of free calcium to join with the oxalate by means of the calcium citrate formation that is relatively soluble. In the dogs with calcium oxalate urolithiasis it has been demonstrated hypocitraturia but the mechanisms responsible for the citrate urinary concentrations decrease are not known.
The increase in the appearance calcium oxalate uroliths can be related to the diets that promote the urinary acidification designed for the prevention of the struvite crystalluria; maybe due to the increase in the quantities of sodium in the diet since major quantities of sodium in the diet promote the excretion of urinary calcium.
The medical handling directed in avoiding the problem relapse, is based on a moderate restriction of proteins, calcium, oxalate and sodium with normal quantities of magnesium and vitamins C and D. To avoid the shortcomings of pyridoxine (Vitamin B6) since this promotes the endogenous oxalate synthesis.
The potassium citrate disables the calcium oxalate crystal formation in human beings for its aptitude to form soluble calcium salts; nevertheless, in dogs this has not been demonstrated nevertheless can be helpful due to its alkaline action. In the dogs the chronic metabolic acidosis, disables the tubular reabsorption of calcium, whereas the metabolic alkalosis promotes the same one. It is preferable to use potassium citrate than sodium bicarbonate like alkalizing agent, since the oral administration of sodium increases the urinary excretion of calcium. It is important to increase the water consumption by the patient, this can be achieved adding some flavor or adding a major quantity of water to the food.
Ammonium Uroliths
The ammonium urate urolithiasis presents commonly in Dalmatians and in patients with portosystemic shunts. The majority of these uroliths are composed by ammonium acid urate, the sodic urate uroliths and uric acid at 100% are in comparison rare. The uric acid is derived from the metabolism of the purines and pyrimidines (dietetic nucleic acids).
The Dalmatian breed presents unique characteristics in contrast to other breeds since they have an ineffective uric acid transport from the blood stream towards the hepatocyte, shortcomings of the uricaze enzyme that oxidizes the uric acid in allantoin, a more soluble compound compared to the uric acid, this conversion takes place inside the hepatocyte. In the kidneys also a shortcoming appears in the membrane transport that reduces the reabsorption of the uric acid leaked in the renal proximate tubes, as well as distal tubular secretion of uric acid, which increase the uric acid and sodic urate (uric acid salt) in the urine. The effect combined of these hereditary abnormalities, is an urinary daily excretion from 200 to 800 mg or more of uric acid, compared to the daily excretion from 15 to 50 mg in the dogs of other breeds.
Only a limited percentage of Dalmatians form urate uroliths, existing a major incidence in the males that in the females (18:1). Only the patients with a daily excretion of uric acid above 550 mg form a group of risk to suffer urate urolithiasis since above this value, the urate starts precipitating. The uric acid solubility constants depends both on the concentration and on the pH, being almost separated to the ionic form to a pH of 6.5 in such a way that the possibility to precipitate is very low, nevertheless below a pH of 6, it is capable of combining with any urinary cation, basically with ammonium and sodium to form urate salts, which have a variable solubility though relatively it lowers a high pH. Nevertheless, the oversaturated solutions of these salts do not precipitate easily in the urine under physiological conditions because they form molecular aggregations and assume the colloidal state l being composed by ammonium and sodium urates, tend to remain in solution because they are of small size and in general they are excreted in the urine. If the ionic urate continues present in the urine, as it happens in the dogs that they excrete big quantities of urates, the molecular attachment increases its size and finally it will precipitate. The mineral crystallization seems to be formed only by the attachment of urate salts more than for the uric acid as in the human beings. The crystallization of the uric acid is favored by the acid pH whereas the alkaline ones predispose the crystallization of urate ammonium acid.
The infections of urinary tract, especially those with urease producing bacteria, can facilitate the crystallization of the ammonium urate on having increased the concentrations of urinary ammonia.
For the control in Dalmatian patients, is important to discard or to confirm the presence of uroliths in the urinary tract, in case of being evident, the surgical extraction must be done and the calculus must be sent for a chemical semiquantitative analysis of the mineral to determine the mineral components of the stone. Nevertheless, in the majority of the occasions it is difficult to obtain the calculus since they are normally in the shape of thin fine sand; if a fair amount is obtained, precipitation must be allowed to withdraw the biggest possible quantity of water and allow its evaporation that will allow the sediment to harden and to send it for analysis.
In case of being few crystals maybe it is necessary to determine the quantity of excretion of uric acid in urine of 24 hours, a normal dog excretes from 15 to 50 mg per day and in case of a Dalmatian with tendency to oversaturation, from 200 to 800 mg per day, the status of active precipitation implies having a oversaturation over 550 mg day.
So the target will be to support the patient below this range to avoid the urine oversaturation with uric acid which can be achieved with two strategies: (1) with therapeutic diets with protein restriction as the ones designed for renal insufficiency and the increase in water consumption and (2) the therapy with inhibiting medicines of the xanthine-oxidase like the allopurinol that avoids the metabolisms of the hypoxanthine to xanthine and from the xanthine to uric acid, with the purpose of taking the excretion of uric acid in 24 hours to a value of 300 +/- 25 mg per day. It is important to not go lower of 275 mg per day with excessive medications of allopurinol since it will be predisposed to crystalluria and xanthine urolithiasis.
It is suitable to take the urinary pH to a range above 7; of being necessary with help of the potassium citrate.
To realize urinary cultures to discard or to confirm infections for urease unfolding bacteria and to implant the antibiotic suitable handling.