Osteoarthritis: Results of Different Treatments during 15 Years in 1126 Dogs and Cats
The aim of the surgeon during the treatment of an osteoarthritic patient is to avoid pain and return to complete joint function through the arthroscopic procedure.
In order to achieve an accurate prognosis the use synovial fluid cytology is recommended, obtaining a synovial fluid sample to perform a histochemical and a cytological examination.
This group was particularly observed in order to learn if any correlation exists between cytology (cellularity, proteins, density, and mucin clotting time) and joint status (pain and function). It is important to know that the result of high cellularity is unpredictable, and the osteoarthritis will be difficult to deal with.
It all depends on the osteoarthritis treatment. In this research, 1126 clinical records were analyzed. The best treatment was found to be the combination of polysulfated glycosaminoglycan** (4 mg/kg IM. every other day for 4 weeks), hyaluronic acid IV *** or IA**** 3 doses every week, and a non steroidal anti-inflammatory drug (Carprofen+, meloxicam++, or etodolac+++).
Preliminary results show a low correlation (r = 0.42, Pearson p<0.05) between synovial fluid cellularity and pain, and a low, negative correlation (r= -0.47, Pearson p<0.05) between synovial fluid cellularity and the return time to joint function. A high negative correlation between pain and recovery time back to full joint function (r = -0.87, Pearson p<0.05) was also found.
So far, no correlation has been found between the other synovial parameters evaluated. This can be due to the high variation existing between dog breeds, pathologies, medical treatments, and the small sample size (n=32).
Although the number of cases analyzed is still relatively low, at this time the cellularity of the synovial sample could be used as a preliminary prognosis tool to predict how long recovery will take. We expect that as more samples from specific groups are analyzed (specific pathology, dog characteristics, etc), synovial fluid analysis will be more and more used as a routine prognosis tool in osteoarthritic dogs.
** Adequan IM Luitpold Pharmaceuticals, Inc. Animal Health Division.
*** Legend ® IV Bayer Laboratories.
****Hylartil ® V. Pharmacia & Upjohn.
+ Rimadyl. Pfizer Laboratories.
++ Metacam ®. Boehringer Ingelheim.
+++ Etogesic. Fort Dodge Laboratories.
Introduction
One of the most frequent problems found in small animal medicine/surgery is, unquestionably, the osteoarthrosis syndrome. Osteoarthrosis must be considered as a syndrome because of the great amount of clinical signs involved, which result in patient's poor life quality, quickly leading to death. Osteoarthritis presents with a series of clinical signs that the pet owner must recognize from the early months of life of the puppy, with joint dysplasia/trauma, including:
The first owner's complaint can be:
Up to 6 months of age:
1. "my pet is very lazy"
2. "my pet does not like to climb in the car"
3. "while the others play my pet is laying down"
From 6 to 11 months of life:
1. "my pet walks with the head and tail down, and an arched back"
2. "my pet won't jump"
3. "my pet runs like a rabbit"
4. "my pet closes its ankles "
5. "my pet splits its elbows"
From 12 months to 2 years:
1. "there is muscular atrophy"
2. "pain in extension or flexion"
3. "it's mood has changed. Now it is somehow aggressive"
4. "my pet suddenly cries because of pain"
From 2 to 6 years (see Figure 1):
Depending on the osteoarthrosis grade, the patient will show different signs, but if the condition has badly progressed:
1. "joints squeak or click"
2. "tremendous muscle volume decrease"
3. "decreased joint movement range, very painful"
4. "increased joint volume"
| Figure 1. | 
Patient with recent left joint replacement because of severe osteoarthrosis due to hip dysplasia. Notice the abnormal angles in the shanks, knees and hips, tail down, light flexion in the back. |
|
| |
When joint aberrations are not diagnosed early enough, treatment can be of great medical/surgical help. Treatment is preventive, though not curative. Historically, the medical has been based on either steroidal or non-steroidal anti-inflammatory drugs. Nevertheless, these treatments have a numerous side effects. Today, the pharmaceutical industry has invested time and money in the development of cyclooxygenase selective substances for the long-term treatment of chronic osteoarthrosis.
Nevertheless, this is not enough and osteoarthrosis syndrome must be treated from different perspectives, considering:
1. Release of vasoactive amines
2. Changes in synovial fluid volume/properties
3. Hyaline cartilage condition/components
4. Subchondral bone structure
5. Alterations in joint capsule and periarticular/transarticular tendons
In the event of advanced osteoarthritis that cannot be medically controlled, total hip replacement will be the first option, while femur head/neck excision will be option 2 (see Figure 2.)
| Figure 2. | 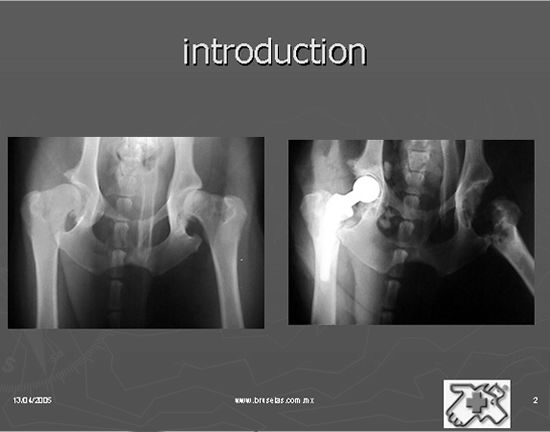
In the event of advanced osteoarthritis that cannot be medically controlled, total hip replacement will be the first option, while femur head/neck excision will be option 2. |
|
| |
Objective
After several years looking for the most appropriate drug or drugs for the treatment of osteoarthritis, an exhaustive revision of osteoarthritic patients was performed in order to evaluate the results, and to learn what the best treatment for each of these pathologies was.
In this study the correlation between synovial fluid and return to good joint function in patients with different levels of osteoarthrosis was established. Today, patients with high genetic value are able to return to reproductive/show activities (See Figures 3 and 4).
| Figure 3. | 
Hermione Villanueva, a multi-best-in-show female Bulldog, champion of the most important world's shows that presented with bilateral cranial crossed ligament rupture. She was away from show rings during the recovery phase from the arthroscopic cranial crossed ligament replacement (a minimum invasion endosurgery). |
|
| |
| Figure 4. | 
Hermione Villanueva had an early recovery. Only 6 months after surgery she was back in the show rings. Today she keeps on winning awards all around. To achieve this, the administration of anti-arthrosis medications was extremely useful for the early recovery of knee normal function, preventing osteoarthritis. |
|
| |
The purpose of this paper is to recognize the tool that is now available, that allows us to determine prognosis, medical/surgical treatments, and to achieve an early joint rehabilitation.
Materials and Methods
From the database of Hospital Veterinario de Especialidades Bruselas SC (Brussels Specialty Veterinary Hospital, HVEB) that includes nearly 8,000 clinical files, 1,126 medical records of patients with osteoarthrosis were obtained. Patients were categorized based on lesions, diagnosis, synovial cytology (only when available), treatment, and prognosis. See Graph 1.
| Graph 1. | 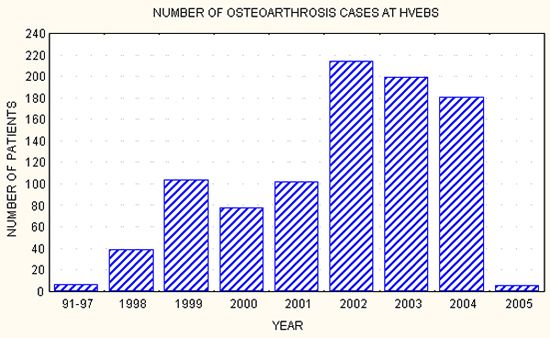
Incidence of osteoarthrosis among HVEB patients, 1998-2005. |
|
| |
Once the 1,126 patients with osteoarthrosis were selected, the following data was collected: File number, owner's name/phone number, patient's name, breed, age, medical/surgical treatment, and whether or not arthroscopy was performed, osteoarthrosis grade, and synovial fluid analytical results. Finally, patient assessment after treatment was also included.
Osteoarthrosis Grading
For osteoarthrosis classification, several factors (i.e., age, weight, breed, duration, and type of joint) must be considered (See Figure 5).
| Figure 5. | 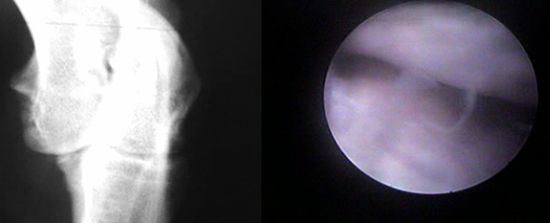
Radiographic/arthroscopic correlation of osteoarthrosis. Seven-month-old Labrador retriever with right, medial, coronoid fragmentation. Fragmentation can be seen in the radiographic study. During arthroscopy, osteochondrosis with very mild chondromalacia was observed (Grade I osteoarthrosis). |
|
| |
Osteoarthrosis resulting in an elbow with joint incongruence could be different from that resulting in an unstable knee. Nevertheless, all osteoarthrosis cases fulfill the same steps at different times, depending on patient's age/weight. The speed of osteoarthrosis development varies. It will be different in a 6-month-old Labrador retriever from that in a 6-year-old English bullmastiff. Likewise, differences will be seen if the lesion is found in an elbow or in a knee.
In these hypothetical cases, the medial coronoid process lesion in the elbow of the 6-month-old Labrador retriever will be radiographically and arthroscopically different from the coronoid process fragmentation of the 6-year-old English bullmastiff.
Radiographically, the Labrador retriever will show minimum changes (from total lack of radiographic changes to joint incongruence of the fragmented process, bone sclerosis), and regular arthroscopic changes (new blood vessel formation in ligament insertions, blood vessel proliferation in capsular insertions progressing towards the joint surface, chondromalacia, intraarticular hemorrhage with yellow-to-red color prevalence). On the other hand, the bullmastiff will show severe radiographic changes of osteoarthrosis (enthesophytosis, osteophytosis, architectural abnormalities in the bone surface border and shape, also affecting the periarticular zone). Arthroscopic differences (eburnation, hemorrhagic zones, mature synovial proliferations, prevalence of a red-to-purple color) will also exist.
This way, arthroscopic grading of the joint lesions can be performed.
| Grade I. | 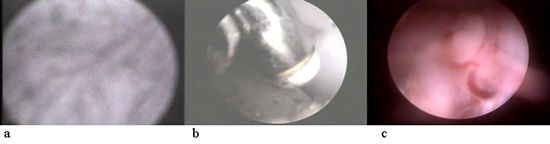
a. Capsular blood vessel proliferation
b. Vaporization of synovial proliferations and chondromalacia
c. Congested synovial proliferations |
|
| |
| Grade II. | 
|
|
| |
Blood vessel active proliferation through synovial (capsular) proliferations not longer exists. Changes in the joint surface are evident with osteochondrosis (i.e., cartilage edema). Chondromalacia and osteophytosis are starting. Non-joint intracapsular surfaces are hemorrhagic, with a dark-red-to-blue color.
| Grade III. | 
a. In osteoarthrosis Grade III the joint capsule shows fibrous proliferations that can be included in joint spaces, ligament insertions, and they can even hide osteophytes. When inspecting a joint with advanced osteoarthrosis, using of an exchange rod to palpate all these capsular proliferations and releasing all possible hidden free osteophytes is recommended.
b. After observing the fibrous capsular surface, observing the subchondral bone (eburnation) will show the incongruence, osteophyte instability, or erosion for a long period of time.
c. Ulnar surface. The medial coronoid fragmentation in an 8-year-old tigress shows active hemorrhages on the joint surface with advanced eburnation. |
|
| |
Synovial fluid assessment
Thirty two (32) synovial samples from 62 different arthroscopic procedures were evaluated. Cellularity, protein, density, mucin coagulation time, and several other parameters were determined in order to evaluate their possible clinical relevance as correlated with patients' final outcome.
Antiarthrosis treatment types
1. Carprofen + 4.4 mg/kg e/24 h, 30-60 days PO.
2. Etodolac ++ 10 mg/kg e/24 h, 30-60 days PO.
3. Meloxicam +++ 0.1 mg/kg e/24 h, 30-60 days PO.
4. Any of the above, with sodium hyaluronate***, 10 mg/20 kg with a maximum of 20 mg/dog and 5 mg/cat e/7 days, for a total of 3 IV applications.
5. Any of 1, 2, or 3 with 4 (above), plus 2 mg/kg polysulfated glycosaminoglycan ** 2 weekly applications for 4 weeks.
6. Any of 1, 2 or 3 with 5 (above) plus high density sodium hyaluronate **** at a dose rate of 0.2-1 ml depending on joint size.
7. In patients subjected to the arthroscopic procedure, any of 1, 2, or 3 plus 6 (above) in the first application, followed by 1, 2, or 3 plus 4 in the two subsequent applications.
Post-treatment patient evaluation
The owners of all treated patients were contacted and questioned for their opinion about treatment result, and whenever possible, medical assessment was performed using Braden's grading method.
Client evaluation included the following questions:
1. How is the patient doing after treatment?
a. Excellently
b. Well
c. Fairly
d. Poorly
e. Very poorly
2. Which of the legs is/was lame? Remember?
a. Yes
b. No
If answer to question 1 was a or b, and if answer to question 2 was b, then the patient has a score of 100%. If answer to question 1 was c, and answer to question 2 was a: then question number 3 was asked:
3. Is there lameness?
a. Yes, mild, with relapse
b. Yes, with relapse 3-4 times per year
c. Yes, it is continuous. Only improves with treatment
d. Yes, lameness is always present. No weight bearing.
If answer is a, then grading is 85%. If answer is b, then grading is 60%. If answer to question 1 was d; answer to question 2 was a; and answer to question 3 was c, then grading is 50%.
Same as e except that answer to question 3 was d. Then grading is 30%.
Results and Discussion
Once all data was gathered from all the HBEV records, patients' review, and telephone survey, all collected results were subjected to simple statistical analysis and, when pertinent, to different correlation specific statistical tests.
Osteoarthrosis grading
This allows for grading osteoarthrosis treatment response with little suggestive involvement:
|
Grade I |
Osteoarthrosis with adequate response to treatment: 85-100% owner satisfaction. |
|
Grade II |
Osteoarthrosis with partial response to treatment: 60-85 % owner satisfaction. |
|
Grade III |
Osteoarthrosis with con little response to treatment: 30-60% owner satisfaction. |
|
Grade IV |
Osteoarthrosis with no response to treatment and no owner satisfaction. |
Antiosteoarthrosis treatment
The study of antiosteoarthritic drugs has now attracted special interest. For more than 15 years, various attempts to offer the veterinarian with panacea-type medications including NSAIDs, leukotriene inhibitors and some neutraceutics were made. Most of these drugs are not bad, but they have the great disadvantage that the owner of the arthritic patient does not see positive results before 6 months of recommended use. This way, treatment is forgotten and-even though this might not be true-the owner thinks that products are useless. The pharmaceutical industry should think about more user-friendly medications. The advantage of administering the drug once per day is now a reality. A single-medication, integral antiosteoarthrosis might exist in the near future. Products for monthly application would be magnificent.
Osteoarthrosis treatment has evolved throughout the years. A 1997-2000 medical record revision showed a very low level of client satisfaction, with a high level of incurable surgical patients. Today, surgery can be prevented by pain control.
Even though osteoarthrosis is a chronic, silent syndrome, it is not completely mute. Therefore, the owner and the practitioner must be familiar with the early stage of osteoarthrosis: the silent stage.
For more than 5,000 years, it has been known that cure from chronic diseases is slow. This is also valid for the osteoarthrosis patient. The great advantage of modern, selective cyclooxygenase drugs (COX) can be used for extended periods of time (minimum 3-6 months) and even for life.
Trying to classify the different grades of osteoarthrosis is a hard task. In the beginning we attempted to learn which the right treatment for osteoarthrosis is. We must understand that osteoarthrosis starts with joint instability/incongruence, changes in the synovial membrane, and abnormal production of synovial fluid (instability), or changes at the joint surface level, such as fibrillation, chondromalacia, eburnation, and cartilaginous metaplasia on the joint surface. As its name suggests, osteochondrosis affects the subchondral portion, so that both collagen and proteoglycans will be altered. Sometimes this triggers the initiation of osteoarthrosis (joint incongruence).
When vasoactive amines are released (inflammation), joint surface changes are seen (glycosaminoglycans), and lack of lubrication/nutrition on the joint surface (hyaluronic acid) occurs, we must think about correcting these changes and treatment should be started including nutritional joint lubrication (hyaluronic acid) to combat osteoarthrosis, joint function improvement (glycosaminoglycans) and a NSAID.
Many of these drugs are available, even though not all of them do what is published with no scientific support. Therefore, after trying different anti-inflammatory drugs, glycosaminoglycans and hyaluronic acid products, those with outstanding effects are mentioned in the paper.
Some drugs with advantages and disadvantages--like high density hyaluronic acid-have a much more evident effect than low density hyaluronic acid. The disadvantage is that high density hyaluronic acid is applied only intraarticularly, and it must be used in patients with arthritis in one or two joints. The advantage (but with no similar effects) of lower density hyaluronic acid is its IV administration with multi-joint effects. Another advantage is that this drug is the first option for patients with ankylosing spondylosis with columna vertebralis multiarthritis.
| Graph 2. | 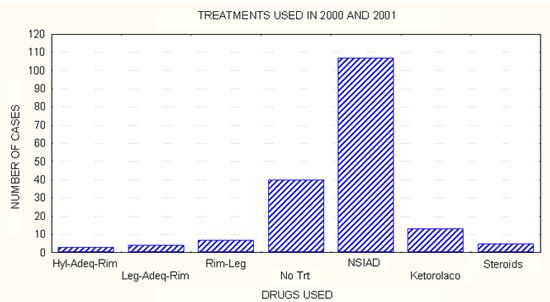
NSAIDs displaced steroidal anti-inflammatory drugs until ten years ago. Nevertheless, until 5 years ago, they were always the best option. Today, the hyaluronic acid-glycosaminoglycan combination has synergistic effects for osteoarthrosis-related pain relief. |
|
| |
| Graph 3. | 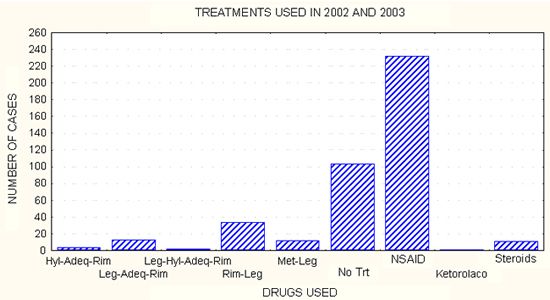
Clinically, client satisfaction starts with the hyaluronic acid-polysulfated glycosaminoglycans combination with carprofen/meloxicam/etodolac. |
|
| |
| Graph 4. | 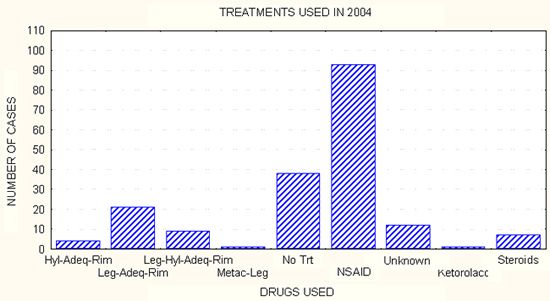
Notice the great increase in Legend's columns, polysulfated glycosaminoglycans and carprofen. |
|
| |
| Graph 5. | 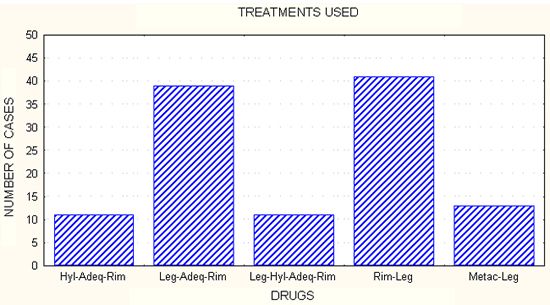
High density hyaluronic acid in combination with low density hyaluronic acid, polysulfated glycosaminoglycan and carprofen/meloxicam are the treatments mostly used for osteoarthrosis control. |
|
| |
| Graph 6. | 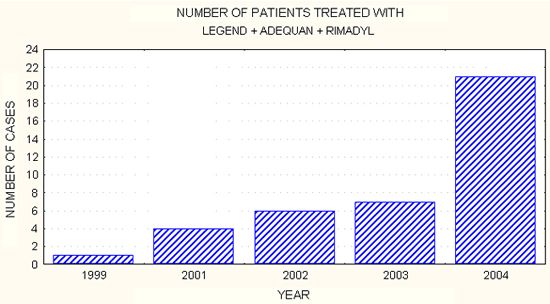
After 3 years of use, the osteoarthrosis integral treatment has shown its effectiveness great degree of arthritic pet owner acceptance. This treatment can be expensive for heavy patients, but given its benefits and good outcome, the owner now prefers it and accepts is more easily. |
|
| |
| Graph 7. | 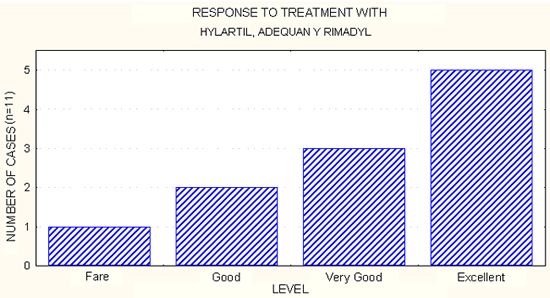
The telephone/personal survey, together with patient clinical orthopedic examination, reveals that response to treatment with Hylartil, Adequan and Rimadyl has been from very good to excellent in most patients. |
|
| |
| Graph 8. | 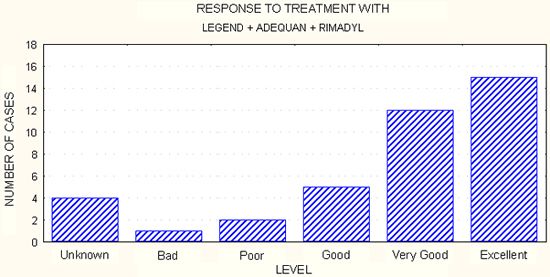
The telephone/personal survey, together with patient clinical orthopedic examination, reveals that response to treatment with Hylartil, Adequan and Rimadyl has been from very good to excellent in most patients. |
|
| |
The osteoarthritis syndrome includes other factors that must be treated:
1. Nutritional:
a. Excess weight must be treated
b. Antioxidants (equilibrium ages)
c. Morbidity support with royal canine-Waltham
d. In the event of excessive overweight, an Obesity Royal Canine Diet must be used, together with a nutraceutical supplement like ol trans (Holiday Laboratories).
Synovial Fluid Cytology/Histochemistry
So far, no correlation has been found among the other parameters evaluated. Even though the number of cases analyzed is still relatively low, synovial fluid sample cellularity can be used as a prognosis tool in order to know whether the patient will recover acceptable joint function. We will continue to obtain samples from specific groups to be analyzed.
Synovial fluid analysis can be performed routinely as an aid in the prognosis of osteoarthritic dogs.
| Graph 9. | 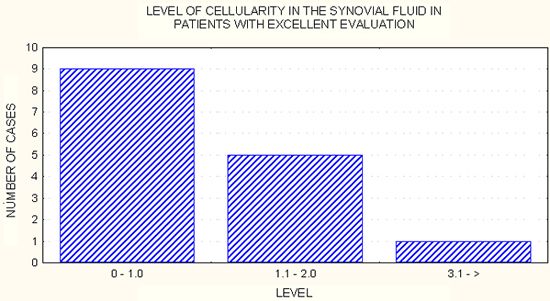
Cellularity in 109/L. Patients with cellularity lower than 2.0 109/L have a good prognosis to recover joint function. |
|
| |
| Graph 10. | 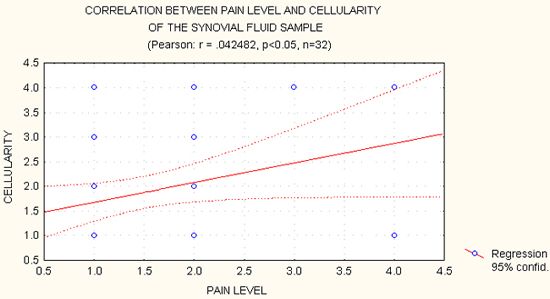
Positive correlation exists between pain and synovial fluid cellularity, meaning that patients with higher levels of pain have a higher amount of white cells in the synovial fluid. |
|
| |
| Graph 11. | 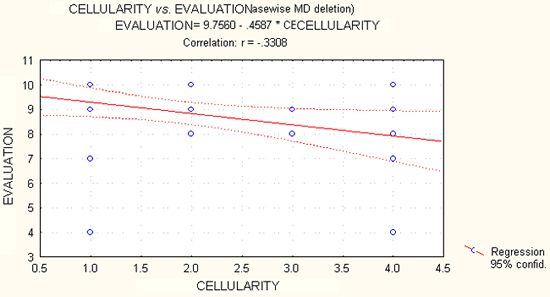
The negative correlation between cellularity and final patient evaluation means that the higher the cellularity the lower the return to function. |
|
| |
| Graph 12. | 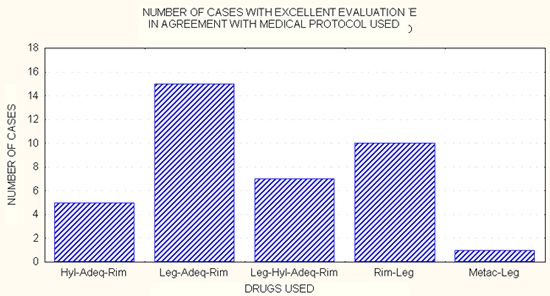
Up to the year 2000, 22% clients showed satisfaction with osteoarthrosis treatment. After 2002 35% pet owners showed satisfaction with osteoarthrosis treatment. In 2005, percent satisfaction has increased to 85%. |
|
| |
1. Osteoarthrosis is a syndrome--or a series of clinical signs--that results in patients' poor life quality, pain, and early death.
2. Rapid recovery and early ambulation was a very popular slogan in the 70's by a Swiss group studying fracture fixation. Throughout the years this technique has been widely distributed/&accepted throughout the world. Today, orthopedics wants to achieve this not only with fractures, but also with osteoarthrosis syndrome.
3. After 20 years of attempts, the use of minimum invasion surgery (arthroscopy) is finally spread throughout the world as the first tool to achieve this.
4. An osteoarthrosis grading method has been created as an aid for a more precise prognosis.
5. The intraarticular or IV application of hyaluronic acid in the polyarthritic patient is combined with polysulfated glycosaminoglycans and NSAIDs (the so-called integral antiarthrosis treatment). This is the recommended treatment to handle chronic joint pain.
6. Synovial fluid analysis can be used to obtain a more precise prognosis about the functional future of a joint. Even though this study shows a positive trend, evaluating a larger number of samples is recommended.