Hamish R. Denny, MA, Vet MB, PhD, DSAO, FRCVS
Tendon structure
Tendons consist of tightly packed bundles of collagen fibres (or fibrils) which surround parallel rows of tendon fibroblasts which are responsible for fibre synthesis. The collagen fibres and cells are packed into fascicles. Although the fibres in the fascicle are essentially parallel, examination of the collagen fibres under polarised light shows evidence of a planar waveform or symmetrical crimp morphology. The crimping provides considerable lateral cohesion in the tendon and this together with the interfibrillar ground substance makes slippage between the fibrils difficult. The organisation of tendon structure allows non-linear load deformation when subjected to tension; the crimp straightens under stress and recoils to its normal position when the load is removed. The tensile strength of the tendon is similar to bone and is able to resist much higher loads than are ordinarily demanded. The collagen bundles are surrounded by peritendon and the epitendon surrounds the entire tendon unit. Both these connective tissue elements carry blood vessels to the internal structures of the tendon. Non-sheathed tendons are covered by the paratendon (loose connective tissue) which allows the tendon to glide and also supplies the blood vessels. When the tendon crosses a joint it is surrounded by a sheath. The tendon sheath consists of a sac containing synovial fluid folded around the tendon, the fold is formed by the mesotendon which carries the blood supply.
Tendon injury and healing
When a tendon is subjected to loads above the safe limit (a tendon of cross-sectional area of 1 cm2 will normally support a load of 600-1000kg), then there is loss of lateral cohesion with slippage and rupture of fibrils. Fibre rupture is associated with severe capillary haemorrhage with in the tendon. There is immediate fibrin deposition and ischaemia at the site of injury, which produces congestion, fibroblast necrosis and fluid accumulation between the fibres. The acute inflammatory exudate also contains hydrolytic enzymes which cause further damage to the collagen fibrils and interfibrillar matrix. Healing following severe tendon injury involves the formation of granulation tissue and the sequence of events is detailed below.
When a tendon is cut, the wound is invaded by fibroblasts from the inner tendon sheath, or, if the wound involves a non-sheathed area of tendon, then the fibroblasts are derived from the paratenon. The fibroblasts lay down randomly orientated collagen fibres in the gap between the severed tendon ends. These fibres then become organised so that by 3 months post injury they are found to be longitudinally orientated between the severed tendon ends. The organisation of orientation is controlled by the directions of strain within the healing tissues.
Investigations into the tensile strength of tendons during the healing process have shown that function of the tendon during the early stages of exudation, fibroplasia and fibrous union has a deleterious effect on healing, whereas function of the tendon during the latter stages of maturation and organisation accelerated the process. Consequently, following tendon repair complete immobilisation is essential for 4-6 weeks postoperatively and then a gradual increase in movement is allowed during the following 2 months. In tendon repair, restoration of tensile strength is the prime objective, but at the same time gliding function should be maintained if normal limb function is to continue. Gliding function of the tendon is commonly compromised by excessive scar tissue formation, this can be minimised by controlled exercise during the latter stages of healing.
Types of tendon injury: Strains and ruptures (tendinitis)
Injuries to a muscle tendon unit (MTU ) are called strains. Injury to any part of the MTU, i.e., the tendon of origin, the muscle belly, or tendon of insertion, will result in dysfunction of the unit as a whole. Strains can be classified as:
 First degree ( mild)
First degree ( mild)
Second degree ( moderate)
Third degree ( severe injury)
The majority of strains resolve with conservative treatment. In the acute phase the aim of treatment is to limit the haemorrhage, fibrin exudation and tissue fluid and this reduces the extent of subsequent scarring and contracture. Treatment will therefore involve the use of cold compresses, immobilisation and prevention of further tensile stress. Examples of strain injuries are listed below:
Strain of the tendon of insertion of the flexor carpi ulnaris, strains of the semitendinosus and sartorius muscles, common calcaneal tendon, and digital flexor tendons, which are seen particularly in the racing Greyhound
Bicipital tenosynovitis
Contracture of the infraspinatus and /or supraspinatus muscles
Quadriceps contracture
Gracilis muscle contracture
Complete ruptures, especially those involving the musculotendinous junction or tendon require surgical repair. Examples of these include:
Gracilis muscle rupture in the racing Greyhound
Gastrocnemius muscle rupture
Severed tendons and tendon ruptures
When treating a minor cut in a region where tendons are relatively superficial, e.g., the plantar aspect of the metatarsus, tendon injuries can be easily overlooked, especially when the main concern with many such wounds is the control of haemorrhage. It is important that the integrity of local tendons is ensured by observing paw/limb position during weight-bearing and that, if injury is suspected, the wound is inspected thoroughly (often requiring the defect in the skin to be enlarged). This is important since early repair of a tendon injury leads to far fewer complications when compared to delayed attempts at treatment. Monofilament nylon sutures are used for repair. The suture patterns include the traditional Bunnell tendon suture (Figure 1), The Pennington locking-loop suture (Figure 2) and the three-loop pulley (Figure 3). The Pennington suture is easier to apply and allows accurate apposition of the tendon ends.
However, the three-loop pulley pattern has been shown to provide more support, less tendon distraction, and less tendon matrix constriction and distortion than the locking-loop pattern. In general, the Pennington locking loop is used for apposing the severed ends of flat tendons, whilst the three-loop pulley is used for round tendons. In chronic tendon injuries filamentous carbon fibre or polyester is used as a scaffold to induce collagen formation and bridge the gap in the tendon. Immobilisation of tendon repairs is essential for some 4-6 weeks postoperatively.
Examples of severed or ruptured tendons and the type of support used following repair include:
Digital extensor tendons (splint following repair)
Digital flexor tendons (flexion bandage or cast following repair)
Common calcaneal tendon (fix hock in extension with lagged bone screw through calcaneus and distal tibia, remove screw after 6 weeks)
| Figure 1. | 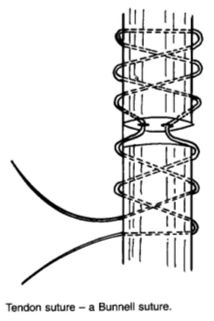
|
|
| |
| | Figure 2. | 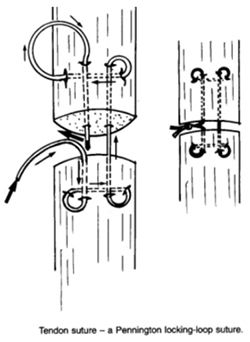
|
|
| |
|
| Figure 3. | 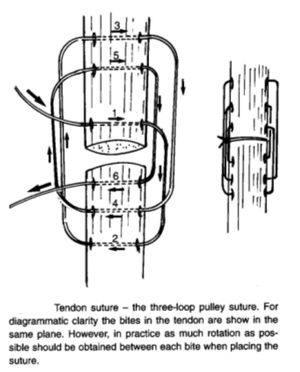
|
|
| |
Tendon avulsions
Most tendon avulsions, except common calcaneal tendon avulsions, tend to be seen in immature dogs and result in the tendon being pulled away from its point of attachment with a fragment of bone. The tendon is reattached with a lagged bone screw placed through the bone fragment. If the fragment is too small to take a screw then a staple or a screw and spiked washer are used to reattach the tendon to the bone. Alternatively, the tendon can be sutured to the adjacent soft tissues.
Examples of tendon avulsions include:
The various avulsion fractures, i.e., scapular tuberosity, olecranon, tibial tuberosity, etc. (Kirschner wires + tension band wire are used for fixation)
Avulsion of the medial epicondyle of the humerus
Avulsion of the long digital extensor tendon in the stifle
Avulsion of the insertion of the gastrocnemius tendon from the calcaneus. This injury tends to be seen as a chronic problem in older Dobermann Pinschers. The hock is temporarily fixed in extension with a lagged bone screw for 6 weeks to allow healing to occur in partial avulsions. In addition, in complete avulsions the tendon is reattached to the calcaneus by passing suture material though the tendon and a transverse tunnel drilled through the calcaneus.
Displaced tendons
Specific examples of this type of problem include:
Displacement of the superficial digital flexor tendon of the calcaneus as a result of rupture of the medial retinaculum. The torn retinaculum is sutured or in chronic cases tightened by an overlap procedure.
Displacement of the tendon of origin of the biceps brachii muscle following rupture of the transverse humeral ligament. The tendon can be retained in its normal position by reconstruction of the ligament with a wire prosthesis or by placing a screw with a smooth shank protruding on the medial edge of the bicipital groove to act as a barrier against tendon displacement.
References
1. Berg, R.J.& Egger,E.L. (1986) In vitro comparison of the three loop pulley and locking loop suture patterns for the repair of canine weight bearing tendons and collateral ligaments. Veterinary Surgery, 15, 107-14.
2. Bunnell, S. (1940) Primary repair of severed tendons. American Journal of Surgery, 47, 502-10
3. Ham, A.W.& Leeson, T.S. ( 1961) Histology, 4th Edition, pp 488-507. JB Lipincott, Philadelphia, PA.
4. Jann, H.W., Stein, L.E. & Good,J.K. (1990) Strength characteristics and failure modes of locking-loop and three loop pulley suture patterns in equine tendons. Veterinary Surgery, 19, 28-33
5. Pennington, D.G. (1979) The locking loop tendon suture. Plastic Reconstructive Surgery, 63, 648-52