May, 2001
Signalment, History, Physical Examination Neurological Examination Tests Performed Case Summary and Diagnosis
Signalment, History, Physical Examination
 Signalment: German shepherd dog, male, 4 years old.
Signalment: German shepherd dog, male, 4 years old.
History: Ten days ago began holding left pelvic limb in flexion, now has progressively worsening ataxia and head tilt.
Past Medical History: No history of previous trauma or illness was reported by the owners.
Medications: Prednisone was given but discontinued because of diarrhea.
Physical Examination
General: Alert and responsive, body condition score 5 / 9
Body weight 28 kg, rectal temperature 102.0; heart rate 120/m; rhythm regular with femoral pulses equal and synchronous. Respiratory system: panting, eupneic. Mucous membranes pink, capillary refill time < 2 sec.
Integument: No abnormalities noted.
Eyes, ears, nose and throat: No abnormalities noted.
Cardiopulmonary, abdominal cavity, musculoskeletal, lymph nodes: No abnormalities noted.
[Top]
Neurological Examination
Consciousness: Alert, responsive.
Posture: N/ Falling, rolling: Absent/ Righting reactions: N Head Tilt, left Tremor: None
Circling: None observed
Gait:
See video

Postural and Placing Reactions
Proprioceptive placing and visual and tactile placing:
 thoracic limbs: unable to evaluate;
thoracic limbs: unable to evaluate;
pelvic limbs: unable to evaluate
Hopping, hemistand/walk
Thoracic limbs: left: slow; right: N;
pelvic limbs: left: slow; right N
Wheelbarrowing
thoracic limbs: unable to evaluate;
pelvic limbs: unable to evaluate
Spinal (segmental) reflexes: (N=normal; D= depressed; A= Absent; I= increased;)
Forelimbs:
Tendon Reflexes: Extensor Carpi: N: Biceps brachii: N; Triceps brachii: N
Flexion Reflexes: N
Crossed Extensor Reflexes: Absent clinically
Pelvic limbs:
Tendon Reflexes: Quadriceps: N; Gastroc/Dig. flexors: N.
Crossed Extensor Reflexes: Absent clinically
Perineal Reflexes: N
Cutaneous Trunci Reflexes: Present in all normal segmental levels.
Painful Stimulation: Normal withdrawal responses.
Cranial Nerves
I: Not tested
II: Vision apparently normal.
III, IV, VI: Pupils equal, normal direct and indirect pupillary light reflexes. Normal ocular positions and movements.
V: Normal
VII: Normal
VIII: (Left head tilt). Physiological Nystagmus: N; Spontaneous nystagmus: absent; Positional horizontal nystagmus with fast phase to the left; Audition apparently normal.
IX, X, XI: Normal swallowing action in response to stimulation.
XII: Tongue: Normal position, symmetry, movements.
[Top]
Tests Performed
Hematology, Chemistry and Urinalysis
Clinical Chemistry Laboratory Results
|
Constituent |
Patient's Results |
Units |
Reference Range (Dog) |
|
Alk. Phosphatase |
47 |
U/L |
15-127 U/L |
|
ALT (SGPT) |
58 |
U/L |
19-70 |
|
Ammonia |
|
mg/dl |
0-92 |
|
AST (SGOT) |
69 |
U/L |
15-43 |
|
Bile acids: |
|
fasting |
|
micromol/L |
0-12 |
|
post-prandial |
|
micromol/L |
0-16 |
|
Bilirubin: direct |
|
mg/dl |
0-0.1 |
|
Bilirubin: total |
0.4 |
mg/dl |
0-0.4 |
|
Blood urea nitrogen (BUN) |
20 |
mg/dl |
8-31 |
|
BUN/creatinine ratio |
20 |
|
6-25 |
|
Calcium |
10.2 |
mg/dl |
9.9-11.4 |
|
Cholesterol |
249 |
mg/dl |
135-345 |
|
Creatine kinase |
|
U/L |
46-320 |
|
Clotting: |
|
PT |
|
SEC |
7.5-19.5 |
|
PTT |
|
SEC |
9-12 |
|
PIVKA |
|
SEC |
15-18 |
|
FDP |
|
|
<10 |
|
Creatinine |
1.0 |
mg/dl |
0.8-1.6 |
|
Glucose |
89 |
mg/dl |
70-118 |
|
Electrolytes: |
|
Anion gap |
10 |
mmol/l |
12-25 |
|
Chloride |
117 |
mmol/l |
105-116 |
|
CO2, total |
21 |
mmol/l |
16-26 |
|
Potassium |
4.0 |
mmol/l |
4.1-5.3 |
|
Sodium |
144 |
mmol/l |
145-154 |
|
Lipase |
|
U/L |
0-500 |
|
Magnesium |
|
mg/dl |
1.2-2.4 |
|
Phosphorus, inorganic |
3.7 |
mg/dl |
3.0-6.2 |
|
Proteins: |
|
Albumin |
3.3 |
g/dl |
2.9-4.2 |
|
A/G ratio |
1.03 |
|
0.6-1.2 |
|
Globulin |
3.2 |
g/dl |
2.3-4.4 |
|
Total protein |
6.5 |
g/dl |
5.4-7.4 |
|
Thyroid: |
|
Thyroxine T4 |
|
micrograms/dl |
1.0-3.6 |
|
Free T4-EQ.D. |
|
ng/ml |
1.0-3.5 |
|
TSH-Canine |
|
mU/L |
2-30 |
|
Tri-iodothyro. T3 |
|
ng/dl |
75-150 |
|
Triglycerides |
|
mg/dl |
19-133 |
Hemogram Results
|
Parameter |
Patient's results |
Reference Values (Dog) |
|
Erythrocytes |
6.93 |
5.5-8.5 million |
|
Hemoglobin (Hb) |
17.2 |
12.0-18.0 g/dl |
|
Hematocrit |
48 |
37-55% |
|
Mean corpuscular volume |
69.3 |
62-77 fl |
|
Mean corpusc. Hb |
24.8 |
33-37 g/d |
|
Mean corpusc. Hb conc. |
35.8 |
21.5-26.5 pg |
|
Reticulocytes |
- |
0.5-1 % |
|
Leucocytes |
10300 |
6000-17000/microliter |
|
Band |
|
0-300/microliter |
|
Neutrophils |
6859 |
3000-11500/microliter |
|
Lymphocytes |
2325 |
1000-4800/microliter |
|
Monocytes |
465 |
150-1350/microliter |
|
Eosinophils |
651 |
100-1250/microliter |
|
Basophils |
0 |
Rare |
|
Platelets |
348,000 |
200-500x1000 |
|
Icteric Index |
|
2.0-5.0 |
|
Plasma proteins |
7.4 |
6.0-8.0 |
|
Fibrinogen |
300 |
200-400 mg/dl |
|
Protein:fibrinogen |
|
>15:1 |
Imaging
Results of Thoracic Radiographs: Ventrodorsal and lateral views of the thorax revealed no abnormalities.
Magnetic Resonance Imaging
| Selected views from Magnetic Resonance Imaging (MRI) | 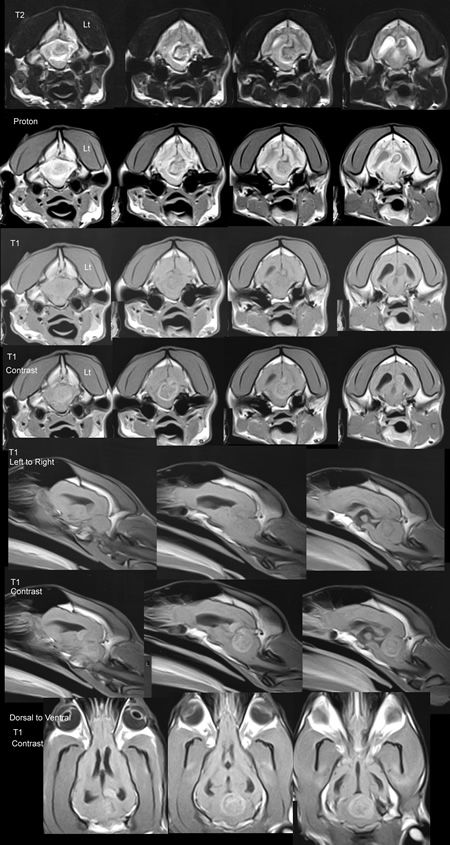
|
|
| |
[Top]
Case Summary and Diagnosis
The clinical presentation and imaging studies in this patient were consistent with a left-sided central vestibular syndrome. The clinical signs were caused by a space consuming mass in the caudal fossa which was evident on imaging and identified at necropsy as a chondrosarcoma.
The patient had head tilt to the left, positional nystagmus with the fast phase to the left, disequilibrium (drunken, staggering gait) and marked hypermetria in the left thoracic and pelvic limbs (Video). The left hypermetria helped identify the vestibular syndrome as central. The clinical localization was supported by the MRI, which clearly demonstrated a large lesion in the left side of the caudal fossa. (MRI results)
Histopathology (VNN is grateful for the participation of Drs. Pesavento and Higgins of the UCD-VMTH Pathology Service in the diagnosis of this case. Their complete report is included below.) Microscopic examinations revealed a mass composed primarily of neoplastic cells embedded in or clustered around variably sized, often large, islands of cartilage. The mass was well demarcated but unencapsulated and composed of cells that were stellate to polygonal, with ample, eosinophilic cytoplasm and poorly defined cell borders. Nuclei in the neoplastic population were round to oval, amphophilic, with finely clumped chromatin and one or two prominent nucleoli. In densely cellular areas the cells were often separated slightly by fibrillar to homogenous, basophilic to eosinophilic material. The islands of cartilage were admixed and occasionally continuous with irregularly shaped, lightly fibrillar, eosinophilic material (osteoid) that often formed anastomosing trabeculae. The pathologic diagnosis was chondrosarcoma.
Chondrosarcomas of the skull base are uncommon, slow-growing tumors in people. Approximately 7% of chondrosarcomas affect the head and neck region in people. CT imaging is better than MRI at showing the calcified chondroid matrix; however, MRI is better at determining the extent of the tumor and involvement of vital skull and neural structures. On T 1-weighted images, chondrosarcomas generally have a low to intermediate signal intensity, with high signal intensity on T 2-weighted and proton-density-weighted images. Variable amounts of heterogeneous contrast enhancement are identifiable and if calcified areas are present will shorten the T 1 and T 2 relaxation times. This patient's MRI demonstrated many of these imaging characteristics and had a rim of hypointensity on both T 1 & T 2-weighted images that on histopathology correlated with islands of cartilage and eosinophilic material or osteoid.
Pathology Report
Dr. P.A. Pesavento, DVM, PhD; Dr. R. Higgins, BVSc, PhD
Veterinary Neurology and Neurosurgery is greatly indebted and grateful to Drs. Pesavento and Higgins for providing this pathology report.
Gross Pathology
Three pieces of tissue are submitted for examination. The first is an entire brain and the second is an irregular piece of bone that is 2.0 x 4.0 x 0.2 x 0.5 cm (petrous temporal bone). The third piece is an irregularly shaped piece of firm tissue, approximately 3.0 x 2.0 x 1.5-0.5 cm This tissue is white and firm, roughly triangular in shape and expanded by a tan to white, smooth, nodular mass. On section, the nodular mass is hard, light tan with diffuse hard white foci. Multiple sections of this mass are placed in cassettes A and B. Multiple sections from rostral to the caudal cerebrum are placed into cassettes C-G. All sections are taken from the right side of the brain. The right cerebellum extending from the falx (rostral) to mid cerebellum. When sectioned, there is a hard mass encompassed by cerebellar cortex that is similar to the mass described above (in the tentorium of the falx cerebri). Sections from the rostral and caudal portions of the mass are taken and placed in cassettes J and K, but sections through the middle portion of the mass are prohibited due to the hard nature of the nodule. The bone (petrous temporal) is submitted for decalcification.
Histopathological Summary
Falx cerebri, tentorium: These are sections of a mass composed primarily of neoplastic cells embedded in or clustered around variably sized, often large, islands of cartilage. The mass is well demarcated but unencapsulated and composed of cells that are stellate to polygonal, with ample, eosinophilic cytoplasm and poorly defined cell borders. Nuclei in the neoplastic population are round to oval, amphophilic, with finely clumped chromatin and 1-2 prominent nucleoli. In densely cellular areas the cells are often slightly separated by fibrillar to homogenous, basophilic to eosinophilic material. The islands of cartilage are admixed and occasionally continuous with irregularly shaped, lightly fibrillar, eosinophilic material (osteoid) that often forms anastomosing trabeculae. In four sections of cerebellum there is a mass, similar to that described in slides above that invades and compresses cortical tissue within the right cerebellar hemisphere. There are multiple sections of the cerebral cortex and brainstem with no detectable histological lesions.
Comment
This dog had a chondrosarcoma with invasion and expansion of the falx cerebri and cerebellum. It is unclear from the gross analysis whether these masses were independent or related (and disconnected during gross dissection). Sections of the petrous temporal bone, which appeared irregular and expanded by gross analysis, are submitted for decalcification. In most regions, the neoplastic cells in this tumor were highly productive for cartilage, and in some regions they surrounded bony spicules and sinophilic material interpreted to be osteoid.
[Top]